It is not yet possible to cure cataracts using conservative methods. If the lens becomes cloudy, only surgery will help preserve vision. Is it possible during this operation not only to replace the clouded organ with an artificial one, but also to correct the accompanying refractive errors, we will talk in this article.
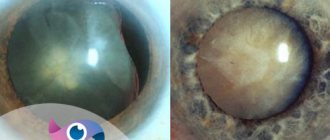
With cataracts, an irreversible process of clouding of the natural lens of the eye, the crystalline lens, begins. The reasons for decreased transparency can be different - from congenital pathologies to traumatic injuries. To date, there is no effective conservative treatment for cataracts; it is impossible to make the clouded organ become transparent again. Therefore, at a certain stage of the disease, the ophthalmologist recommends surgery to replace the natural eye lens with an artificial analogue - an intraocular lens (IOL).
In many patients, cataracts are accompanied by refractive errors - myopia, farsightedness or astigmatism. Modern ophthalmic surgery makes it possible to correct such vision defects during lens replacement surgery.
How to make the right choice?
Some people talk about IOLs as “glasses inside the eye.” This opinion is partly true. The intraocular lens is placed inside the eye, so it is important to prevent its rejection from the ocular tissue, especially from the lens capsule. To achieve this, biologically and chemically inert materials must be used in the process of manufacturing natural lens prostheses. Among them are synthetic polymers.
Also, when studying the issue of choosing a lens, you should remember the importance of the following parameters:
- The size of the optical part of the lens with supporting elements.
- Lens diameter.
- Lens thickness.
Hard lenses differ in the size of the optical part in the range of 5 – 6.5 mm. To this value is added the size of the arms necessary for attaching the intraocular lens to the capsular membrane, iris bursa or ciliary body. As a result, during the operation to implant a rigid IOL, the surgeon makes a 6-7 mm incision, which, of course, is not optimal. In this regard, currently, implantation of rigid IOLs is performed extremely rarely and, as a rule, only for medical reasons.
Simultaneous treatment of farsightedness and cataracts
When these two pathologies are combined, refractive lens replacement is the preferred, and often the only possible option to improve vision. Experts note that such patients have an increased risk of developing closed or narrow-angle glaucoma. If you replace the lens with an artificial implant with individually selected characteristics, you can reduce the likelihood of developing this disease several times. Unlike a natural organ, an artificial one is several times thinner (4.5 mm versus 0.75 mm). When the lens is replaced with an IOL, the angle of the anterior eye chamber, from where the intraocular fluid drains, opens. This reduces intraocular pressure and thereby reduces the risk of glaucoma.
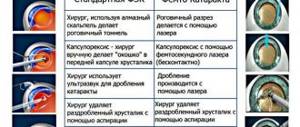
Phacoemulsification - a new word in eye surgery
This surgical treatment of cataracts eliminates the need for severe dissection of the cornea. The maximum incision size is 3 mm. Also, it is allowed to dissect not the cornea, but the sclera.
To carry out phacoemulsification, special flexible IOLs with an elastic structure and miniature size are required. Flexible synthetic polymers are used for their manufacture. Before surgery, such natural lens prostheses are bent in half, so their size does not exceed 3.5 mm. When choosing ultrathin IOLs, you can expect a size of 1.8-2.5 mm. The lens unfolds after implantation, returning to its original size already in the capsule.
If cataracts are treated with extracapsular extraction, rigid IOLs may be used for implantation. In fact, such lenses are quite elastic, so there is no mechanical pressure on the soft eye tissues.
The latter method is used extremely rarely today. In most cases, implantation is carried out with soft prostheses - silicone, acrylic and hydrogel lenses. In this case, flexible intraocular lenses can be divided into two large groups - monofocal and multifocal lenses. A monofocal artificial lens can provide a patient who requires cataract treatment with good vision at only one distance - far or near. And implantation of a multifocal intraocular lens allows the patient to see well at any distance: far, near, at medium distances. However, such IOLs are not suitable for everyone, so a thorough examination is carried out before surgical treatment. The attending ophthalmologist will help you choose a lens for cataracts, who will determine the most optimal option depending on the condition of the eye and the method of surgery.
In conclusion, it should be noted that the production of high-quality IOLs is now established in many European countries. The products (England) and Acrisof (Alcon, USA) are in good standing.
Advice for patients during postoperative rehabilitation
In the first few days after surgical lens replacement, to avoid the development of edema, it is not recommended to sleep on the side of the operated eye. Do not rub the eye; It is advisable not to touch it at all. To prevent possible exposure to dust and direct sunlight while outdoors, you need to protect your eyes with dark glasses. During the first week, it is forbidden to wash your hair, and when taking a shower, you must ensure that water and detergents do not get on your face. Prescribed anti-inflammatory and disinfectant drops must be instilled strictly according to the scheme recommended by the surgeon.
Reading and other activities involving visual concentration can be gradually resumed from the second week. Short-term work at a computer monitor and short viewing of TV are also allowed. In all these cases, at the slightest sign of fatigue (heaviness or dryness in the eyes, frequent blinking, redness of the sclera), you must immediately stop and give your eyes a rest.
If the patient after the operation does not lose motivation to have good vision and healthy eyes, i.e. complies with all instructions and, in particular, does not miss scheduled follow-up visits to the ophthalmologist, then in most cases it is possible to achieve a pronounced and stable therapeutic effect for many years.
Cost of services for cataract treatment
| № | Service name | Price in rubles | Make an appointment |
| 2009003 | Optical-reconstructive intervention in the anterior segment of the eye for cataracts and post-traumatic and post-traumatic changes | 90000 | Sign up |
| 2008047 | Phacoemulsification for complicated, mature and overmature cataracts, category 3 of complexity | 86880 | Sign up |
| 2008046 | Phacoemulsification for complicated, mature and overmature cataracts, category 2 of complexity | 79650 | Sign up |
| 2008045 | Phacoemulsification for complicated, mature and overmature cataracts, category 1 of complexity | 77400 | Sign up |
| 2008044 | Phacoemulsification for initial and immature cataracts, category 3 of complexity | 71220 | Sign up |
| 2008043 | Phacoemulsification for initial and immature cataracts, category 2 of complexity | 67080 | Sign up |
| 2014001 | Penetrating keratoplasty + phacoemulsification or cataract extraction with IOL implantation (complexity category 2) | 96000 | Sign up |
| 2014003 | Penetrating keratoplasty + reconstruction of the anterior chamber with iris plastic surgery, phacoemulsification or cataract extraction with IOL implantation | 120000 | Sign up |
| 2014005 | Deep anterior lamellar keratoplasty + phacoemulsification or cataract extraction with IOL implantation (complexity category 2) | 108000 | Sign up |
| 2014007 | Posterior layered endothelial keratoplasty + phacoemulsification or cataract extraction with IOL implantation | 84000 | Sign up |
| 2008041 | Discision of secondary cataract | 9000 | Sign up |
| 2008053 | A set of consumables and an imported intraocular lens for phacoemulsification of cataracts with cataract removal. | 42000 | Sign up |
| 2008005 | Ultrasound phacoemulsification with IOL implantation for initial and immature age-related cataracts | 79650 | Sign up |
| 2008007 | Ultrasound phacoemulsification with IOL implantation for complicated, mature and overmature age-related cataracts | 84440 | Sign up |
| 2008012 | Cataract removal without phacoemulsification + IOL | 40200 | Sign up |
| 2008021 | Cataract extraction with implantation of an artificial lens of the first category of complexity | 40500 | Sign up |
| 2008022 | Cataract extraction with implantation of an artificial lens of the second category of complexity | 45600 | Sign up |
| 2008023 | Cataract extraction with implantation of an artificial lens of the third category of complexity | 50400 | Sign up |
Making an appointment Today: 14 registered
Correction of myopia during cataract removal
Myopia can be corrected in several ways. The first is when, after removing the clouded organ, an implant with refractive characteristics that completely compensate for myopic disorders is installed inside the eye. Another option is a combination of phacoemulsification (cataract surgery) and laser vision correction. In the second case, after removing the lens, the shape of the cornea is changed using a laser in such a way as to achieve the correct focusing of light on the retina. As a rule, laser correction is contraindicated for people with a high degree of myopia, so such patients are prescribed refractive lens replacement.
What are the types of intraocular lenses?
Intraocular lenses (IOLs) are often referred to as “glasses in the eye,” but this is only partly correct. Glass lenses can only correct visual acuity; intraocular lenses restore it. However, the main difference is that the lenses of the glasses are in front of the eye, and IOLs are always implanted inside the eye. Such lenses should be well tolerated by the surrounding tissues, primarily by the lens capsule. Therefore, intraocular lenses, which are essentially a prosthesis of the natural lens, are made from biocompatible materials. Synthetic polymers are considered the best option for these purposes.
The first operation to implant an artificial lens was performed in 1949 by London ophthalmologist Harold Ridley. It is not surprising that in those days IOL implantation operations were not at all ideal, because their technique had not yet been sufficiently developed. However, the idea of replacing a failed cloudy lens with a corresponding analogue with more advanced optical characteristics began to develop intensively.
In the USSR, the first IOL (Fedorov-Zakharov lens) was developed in 1967. Over the years, the model has been modernized many times and today remains quite in demand. As a representative of the first generation of artificial lenses, the lens does not have the flexibility of current models, but today it is successfully used in Russia and abroad in cataract surgery. For the manufacture of modern rigid intraocular lenses, highly transparent bioinert plastic with a high index of biocompatibility with eye tissues is used.
True, biocompatibility alone is not enough to evaluate an IOL. Three important quantities are also taken into account: the size of the lens and its supporting elements, the diameter of the optical part, and its thickness. And the fact is that the size of the optical part of hard lenses reaches 5 - 6.5 mm. Let's add to this the size of the attachment arms required to fix the lens to the iris, lens capsule and ciliary body, and it turns out that such a lens can only be implanted into the eye by making an incision of at least 6-7 mm.
It is worth mentioning that previously, surgical treatment of cataracts was performed using the method of extracapsular extraction and the size of the IOL was not given decisive importance. One way or another, a small incision was made in the cornea, then the iris was retracted to the side, the failed lens was removed and an intraocular lens was inserted into its capsule. The size of the incision was quite large and implantation of the lens did not present any difficulty. But it was precisely this incision that was a serious drawback of the surgical method. The fact is that the cornea does not have vessels that supply it with blood, and healing occurs very slowly, so it was necessary to put sutures on such an incision. And any suture, even a very thin one, can cause corneal astigmatism, as it disrupts the sphericity of the eyeball.
The desire to avoid this serious complication and the development of medical technology have led to the emergence of a new method of surgical treatment of cataracts - phacoemulsification. This operation is fundamentally different from its predecessor, extracapsular extraction. After all, now there is no need to make a huge incision on the cornea; a puncture incision, the size of which does not exceed 3 mm, is sufficient. Moreover, it can be done not in the cornea, but in the sclera.
This gentle technique became possible with the advent of appropriate acrylic polymers and the manufacture of miniature flexible intraocular lenses from them.
The material they are made of is so soft that it allows the lenses to be bent in half. Therefore, the size of such IOLs before implantation approaches 3-3.5 mm, and there are also ultra-thin artificial lenses, their diameter is even 2.5 mm. When such lenses are inserted into the lens capsule, they unfold independently and take the desired shape.