Keratitis is a general name for a number of diseases of the visual analyzer, the distinctive characteristic of which is inflammation of the cornea of the eye.
Due to the accumulation of infiltrate, cloudiness occurs, which in the case of purulent infection is accompanied by necrosis of the corneal tissue. Pathology can occur either as an independent disease or as a consequence of existing disorders in the body.
Keratitis of the eye leads to decreased visual acuity, glaucoma and even loss of the eyeball. The sooner the patient receives medical assistance, the greater the chance of avoiding undesirable consequences.
This article will help you understand what keratitis is, describe its symptoms and treatment.
Causes of keratitis
Keratitis has a varied etiology. But in most cases (about 70%) the causative agents of the disease are herpes simplex and herpes zoster viruses (shingles). Other reasons include:
- infections: viral (causative agents are: adenoviruses , varicella zoster virus , measles);
- bacterial. Causes purulent keratitis of the eye (pathogens: streptococci , staphylococci , Pseudomonas aeruginosa and Escherichia coli , pathogens of tuberculosis , diphtheria , syphilis);
- fungal (candida, aspergillus, fusarium mushrooms);
- chlamydial infection (chlamydia);
- parasitic (amoeba, leishmania, worms).
Provoking factors for the development of the disease
Factors that favor the development of pathology include:
- vitamin deficiencies;
- decreased immunity;
- disruption of the trigeminal nerve;
- diabetes;
- history of gout.
Diagnosis of keratitis
The diagnosis is made based on a general examination, medical history and a special fluorescein test that uses dyes. In addition, the specialist will examine the eye using a slit lamp, assess the nature and extent of the lesion, check visual acuity and collect material for research using the PCR method - polymerase chain reaction. This way he will determine which pathogen caused the disease. The following may also be prescribed:
- biopsy of eye tissue;
- allergy tests;
- tests for tuberculosis;
- bacterial sowing, etc.
Symptoms of keratitis
The main and common symptom for all keratitis is corneal syndrome. It is characterized by:
- photophobia (photophobia);
- excessive tear production;
- reflex closure of the eyelid (blepharospasm).
Corneal syndrome occurs due to the pressure of the infiltrate on the nerve endings. The accumulation of leukocytes, plasma cells and histiocytes leads to a decrease in the transparency of the cornea, disruption of its shape and clouding.
Against this background, sensations of a foreign body in the eye, discomfort and pain occur. The cornea of the eye becomes rough and turns red (see photo above). Patients note worsening vision.
Symptoms
Having studied the classification, you can see how diverse the symptoms of keratitis in children are, and each of them may indicate a specific form of the disease. Despite these nuances, there are typical signs by which one can recognize the inflammatory process of the cornea at the initial stage of its development. These include:
- photophobia;
- hyperemia (redness) of the conjunctiva;
- lacrimation;
- cutting pain;
- complaints of a foreign body in the eye;
- decreased visual acuity: feeling of a veil, fog before the eyes;
- the vessels on the surface of the eye become bright red and look like a branched tree;
- blepharospasm: involuntary contraction of the eye muscle, which leads to spasmodic closure of the eyelids;
- itching;
- swelling, dryness, clouding of the cornea;
- formation of infiltrate (turbidity), in place of which an ulcer forms over time;
- filamentous mucus in the conjunctival sac.
Sometimes parents worry whether keratitis is contagious or not, since there may be other children in the family, and whether they need to be isolated from the sick baby. Yes, it is transmitted by contact. Many symptoms of keratitis are similar to those of allergic conjunctivitis. Even doctors require multi-stage and thorough diagnostics in order to separate these two diseases and ultimately prescribe the correct treatment. Therefore, modern diagnostics plays an important role here.
Helpful advice. There is a category of parents who, having seen redness or clouding of the mucous membrane of the child’s eye, do not attach much importance to it. They rinse the eye, use the first drops found in the medicine cabinet, thinking that it is due to overwork or insomnia. Any eye problems in children should force parents to immediately consult an ophthalmologist.
Classification of keratitis
Keratitis is classified according to several criteria.
- Due to the occurrence: bacterial keratitis (congenital parenchymal keratitis, the development of which is caused by the causative agent of syphilis, is separately distinguished);
- viral keratitis;
- allergic;
- fungal keratitis;
- caused by protozoa, most often amoebas;
- photokeratitis;
- traumatic keratitis;
- neuroparalytic keratitis, occurs due to damage to the trigeminal nerve;
- unknown etiology (idiopathic keratitis).
- endogenous, or developed due to internal reasons (vitaminosis, rheumatism, allergic reactions, etc.);
- superficial (inflammation is localized in the upper layer);
- central (at the pupil);
Congenital keratitis
Parenchymal keratitis is the extreme stage of congenital syphilis. It manifests itself even after several generations. People under 20 years of age are especially susceptible to it.
The pathology is characterized by cyclicality, bilateral lesions, redness of the choroid and the absence of corneal lesions.
Symptoms of the disease
When the disease begins to develop, the baby may complain of pain in the organs of vision.
It is quite easy to recognize a problem in a child. The first symptoms appear during the first days after infection. The child begins to complain of discomfort and pain in the eyes. As the pathology develops, the manifestations increase. In addition to the symptoms characteristic of inflammation, signs of corneal syndrome appear. This condition is extremely dangerous and requires treatment, otherwise there is a risk of vision loss. Keratitis in children can be recognized by symptoms such as:
- cutting pain in the eyes;
- profuse lacrimation;
- closing of eyelids;
- "veil" effect;
- itching;
- discharge accumulated around the eyes;
- blurred vision.
Further development of the pathology provokes the penetration of infection into the deep layers of the membrane. First, the cornea becomes rough, then an infiltrate forms. The subsequent effect is necrosis of the eyeball tissue and the appearance of ulcers at the sites of epithelial rejection. The most dangerous consequence is the formation of scars and perforation, which is characterized by the penetration of infection deep into the organ.
Diagnostics
Corneal syndrome is the first sign that will help the ophthalmologist diagnose inflammation of the cornea in a patient.
To conduct further research, the specialist instills anesthetic drops into the patient. This will help relieve spasm and open the eyelids.
The next step will be collecting anamnesis, general examination and checking visual acuity.
To clarify the diagnosis, ophthalmologists resort to such additional research methods as:
- biomicroscopy (study of the structures of the visual analyzer using a slit lamp);
- ophthalmoscopy (allows you to evaluate changes resulting from the inflammatory process);
- staining corneal tissue with fluorescein for better visualization of structural changes;
- Ultrasound.
Treatment
Immediate treatment under the supervision of a specialist is necessary for any type of disease. Keratitis is a contagious disease; treatment of sick children is carried out in hospitalization.
To identify the causative agent of the disease, the ophthalmologist examines the patient, prescribing a series of tests. Assistants wash the eyes, take a smear of the infiltrate, and collect a general blood test. After the result is obtained, complex treatment is prescribed.
Ointments and antimicrobial agents
Ointments for keratitis are used once a day at night; it is recommended to drop antimicrobial agents into the eyes at least 4 times.
- 1% erythromycin ointment;
- 1% tetracycline ointment;
- 0.3% ciprofloxacin ointment or solution;
- colistimethate ointment or solution, rolitetracycline;
- 0.01% solution of Miramistin;
- 0.3 solution of lomefloxacin.
Anti-inflammatory
Anti-inflammatory drugs are used to reduce inflammatory processes - 0.1% diclofenac solution, 1 drop 4 times a day. To reduce the risk of internal synechiae, solutions are used: 0.5 cyclopentolate, 1% atropine, 0.5% tropicamide.
Injections
Treatment of keratitis is carried out in conjunction with injections of antibiotics. Treatment is carried out with intramuscular and intravenous injections.
Intramuscularly
The most common and effective treatment is using penicillins . Injections are given at least 5 times a day, sometimes 10 injections can be prescribed.
Intravenously
Intravenous detoxification treatment is carried out with a 5% glucose solution, 200-400 ml of hemodez solution, 2 g of 200-400 ml of ascorbic acid. If healing takes a long time, drugs that stimulate the immune system are prescribed. Treatment is with metronidazole 500 mg per day or every other day.
Treatment of keratitis
Treatment of eye keratitis must be carried out in a hospital and lasts five days. Continues at home if necessary. If a patient has keratouveitis in parallel with keratitis, the symptoms of the disease can persist for up to several months.
Drug treatment
To achieve a speedy recovery, local and systemic therapy is used.
Systemic therapy necessarily implies:
- taking medications designed to destroy pathogens. For purulent inflammation, antibiotics are prescribed (Ciprofloxacin , Ceftriaxone , Moxifloxacin). For viral nature of keratitis - Acyclovir. Fungal keratitis is treated with Voriconazole, Fluconazole, Itraconazole;
- detoxification measures (droppers with saline or Rheosorbilact, drinking plenty of fluids);
- prescribing antihistamines to reduce swelling (Zyrtec, Zodak, Desloratadine).
Additionally, the patient is prescribed aloe extract to improve the trophism of the affected tissues and multivitamin complexes.
Keratitis of any nature requires local treatment. For this purpose, use:
- eye drops containing antibiotics (Tobrex, Floxal);
- eye drops with an antiseptic (Oftamirin, Okomistin, Albucid), which will not only have a detrimental effect on pathogenic microorganisms, but will also prevent the addition of a secondary infection;
- Okoferon drops, if the cause of the disease is a virus;
- Zovirax (ointment), if the causative agent of keratitis is the chickenpox virus or herpes;
- drops with corticoids (Maxidex, Sofradex, Tobradex), which prevent damage to the deep layers of the cornea;
- ointments or gels that accelerate regeneration processes (Lakropos, Korneregel, Vidisik).
Drug treatment of ocular keratitis is usually supplemented with physiotherapy (phonophoresis, electrophoresis, magnetic therapy).
Parenchymal keratitis requires specific treatment. The first stage is preparation - taking iodine preparations, then administering Bioquinol intramuscularly.
The second stage is treatment with penicillin for 14 days. Along with the antibiotic, mydriatics (Atropine, Irifrin, Cyclomed), yellow mercury ointment, dionine solution and corticosteroid drugs are prescribed locally.
Surgery
The indication for surgery is the presence of ulcers on the cornea of the eye. To eliminate tissue defects, modern microsurgery methods are used: laser coagulation and cryoapplication. If a scar has formed, keratoplasty is performed.
Treatment
How much keratitis is treated will depend on the advanced stage of the disease and the timeliness of contacting an ophthalmologist. Parents must strictly follow all his recommendations after confirming the diagnosis. These can be both medications and folk remedies.
Drug treatment
Drug treatment of keratitis in children involves the use of the following drugs:
- ointments (once a day, at night): erythromycin, tetracycline, ciprofloxacin, colistimethate, roletetracycline, acyclovir, Zovirax;
- eye drops (up to 4 times a day): miramistin, lomefloxacin, ciprofloxacin, colistimethate, roletetracycline, diclofenac, cyclopentolate, atropine, tropicamide, ophthalmoferon, poludan, actipol;
- intramuscular injections of penicillin, non-steroidal anti-inflammatory drugs (diclofenac sodium), B vitamins, ascorbic acid;
- NSAIDs can be administered rectally (Voltaren suppositories) or orally (Indomethacin tablets);
- intravenous injections of solutions of glucose, hemodez, ascorbic acid;
- drugs to strengthen the immune system;
- metronidazole;
- at the same time, treatment of diseases that served as an impetus for the development of keratitis is carried out;
- mechanical extinguishing of the ulcer with an alcohol solution of brilliant green, an alcohol solution of iodine, cryo-, thermo, diathermocoagulation;
- laser stimulation, magnetic therapy using 20% Actovegin or solcoseryl gels;
- electrophoresis with lidase and collalysine;
- rinsing with antimicrobial agents;
- therapeutic keratoplasty.
Self-medication of keratitis in a child is excluded, otherwise it can lead to irreversible and dangerous consequences.
Folk remedies
Treatment of keratitis with folk remedies is considered very effective, but they are effective only if they are approved by an ophthalmologist and are used as ancillary to the main course of therapy.
- instillation of sea buckthorn oil, 1% aqueous extract of propolis, woodlice infusion;
- contrast compresses: applying napkins soaked in either cold or hot water to the eyes;
- lotions with infusions of sweet clover flowers, eyebright, calendula, chamomile.
Answers to the question of how long it takes to treat keratitis in children may vary, since the duration of the course of therapy depends on many factors. This includes the general health of the baby, the advanced stage of the disease, and its type. On average, this is 2-4 weeks in a hospital setting. If you don’t catch it in time and consult a doctor, the consequences can be very dire.
Special attention! Very often, recipes for folk remedies against keratitis suggest using garlic or celandine juice. Be aware that they are very irritating to the mucous membrane of the eye and can cause a burn.
Forecast
The outcome of the disease mainly depends on the nature of tissue damage, the location of the infiltrate and the complications that arise.
Therapy at the initial stages of the pathology shows good results - the infiltrate resolves without consequences or minor opacities occur.
If treatment is not provided on time, the outcome of the disease may be:
- thorn;
- glaucoma;
- optic nerve atrophy;
- atrophy of the eyeball;
- loss of visual function.
Consequences
Dangerous complications of keratitis in children can be irreversible if treatment was started too late or parents self-medicated the disease without consulting an ophthalmologist. These include:
- scars on the cornea;
- thorn;
- decreased vision;
- "dendritic ulcers";
- sclerosis of the eye shell;
- constant relapses;
- perforation (formation of a hole) of the cornea;
- blindness.
To ensure that the consequences of keratitis in children are not so dangerous, preventive measures must be taken in time. They will reduce the risk of illness, and if inflammation does begin, its form will not be so severe.
For consolation. Despite the fact that the consequences of keratitis are very dangerous for the health of children, they are diagnosed only in 4-5% of cases. Modern medicine and parental care prevent the development of such terrible complications.
Prevention
For preventive purposes, any child’s illnesses must be diagnosed and treated in a timely manner.
It is necessary to protect your eyes from the penetration of dangerous agents from the birth of your child. Therefore, parents must independently carry out prevention and teach their children to do it. The first step is to conduct annual inspections. If your baby often has ophthalmological ailments, visits to the doctor should be regular. General prevention includes the following measures:
- compliance with hygiene rules;
- eye protection from injuries and burns;
- timely treatment of all diseases;
- exclusion of possible allergens;
- isolation from the focus of keratitis.
If alarming symptoms appear, you should not self-medicate. The symptoms of keratitis are similar to those of conjunctivitis, so without diagnosis there is no need to start therapy. The first disease is considered less common among children. It is important to understand that complications during the development of the disease are extremely dangerous, and the consequences can be irreversible.
Cornea and its properties
The cornea is the surface layer of the eyeball. Normally, the cornea is transparent, has a regular spherical shape, smooth, quite sensitive, and shiny. There are five layers in the cornea.
- Stratified squamous epithelium is the outer layer of the cornea, which has good regenerative abilities.
- Bowman's membrane is a fairly thin, but most sensitive layer due to the nerves located in it. This shell has good resistance to damage and poor resistance to infection. It is not capable of good regeneration, therefore, after its damage, thin opacities remain.
- The cornea's own tissue is the “heart” of the cornea and has sufficient density due to the fibrils intertwined in it.
- Descemet's membrane is homogeneous and is a derivative of epithelium. It easily peels off from the stroma and forms folds. This corneal layer is more resistant to infection than damage and is capable of regeneration.
- The endothelium is the deep layer of the cornea. Damage to this layer leads to the penetration of anterior chamber moisture into the layers of the cornea, disruption of its nutrition and opacities.
The cornea does not have blood or lymphatic vessels.
Metabolism in the cornea to maintain its basic properties is carried out by circulating nutrients from the marginal loop network, which originates from the anterior ciliary artery system. But the sensitivity of the cornea is very high. This is due to a rich network of sensory nerves originating from the ciliary nerves and penetrating into it, the iris and the ciliary body from the suprachoroidal space. In the cornea, the nerves lose their myelin sheath, that is, they become “naked” and become even more unstable to external stimuli.
In addition to local innervation, the cornea has an autonomic nervous system. It is represented by part of the fibers of the trigeminal and facial nerves as part of the zygomatic nerve. Such intense innervation of the cornea determines its high sensitivity and trophism. Therefore, all pathological processes in the cornea are accompanied by quite severe pain. In addition, innervation disorders can lead to eating disorders, and, consequently, to pathology.
The high sensitivity of the cornea and the commonality of its innervation with the eyelids, mucous membrane and lacrimal gland provokes the emergence of a general protective reflex when the cornea is irritated. The manifestation of this reflex is blepharospasm and lacrimation. Eyelid spasm protects the cornea and, together with lacrimation, helps to moisten it and remove foreign bodies. Tear has a beneficial bactericidal effect with lysozyme.
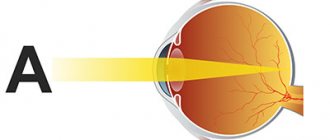
In addition to its protective and moisturizing effect, the cornea has enormous refractive power. The preservation of all its basic properties is the most important in building an image and clear vision.
Exogenous keratitis
The cornea, due to its location in the foreground, is susceptible to traumatic lesions. Keratitis is caused by injuries such as a foreign body of the cornea, erosions, and burns. A gray infiltrate forms around the affected tissue, which, with timely treatment, can be completely cured in 5 to 7 days.
Post-traumatic inflammation of the cornea is common among people in construction professions. Work without observing safety precautions is often accompanied by the entry of foreign bodies of various origins into the cornea. If you do not immediately contact an ophthalmologist to remove the foreign body, the resulting keratitis, even with proper treatment, will leave behind cloudiness.
A purulent infection can penetrate into damaged corneal tissue. As a result, serious purulent inflammation may occur with melting of all layers of the cornea, which can lead to a significant decrease in vision, blindness, and even loss of the eyeball.
One of the dangerous complications of traumatic keratitis is a purulent corneal ulcer.
Prevention and prognosis
The prognosis for keratitis primarily depends on the location and depth of corneal damage. With timely treatment, superficial infiltrates completely resolve or slight opacities remain, which have virtually no effect on visual acuity.
Deep keratitis and ulcers, especially if they are localized in the central and paracentral zone of the cornea, can lead to a significant decrease in visual acuity due to the development of intense opacities and the formation of rough scars.
Prevention of keratitis consists of preventing injuries and microtraumas of the eye, which includes the use of safety glasses, safety precautions in production and construction.
Careful adherence to the rules of wearing and care when using contact lenses is necessary; prevention of contact of various chemicals into the eye, leading to the development of burns of the cornea and mucous membrane of the eye; timely detection and treatment of chronic blepharitis, conjunctivitis; correction of immunodeficiency states. At the initial manifestations of the disease, timely contact with a specialist is the key to successful treatment and preservation of vision.
Endogenous keratitis
Among endogenous keratitis, herpetic keratitis has a special place and widespread distribution . Herpetic keratitis is classified as neurogenic inflammation. The causative agent is the herpes virus (Herpes zoster), “lives” in the trigeminal nerve and can, under unfavorable conditions, migrate along its branches.
Its more well-known manifestations are rashes on the lip. But recently its so-called ocular form has begun to occur quite often. The symptoms of this keratitis are no different from other types of keratitis. But upon examination, infiltrates have their own peculiarity.
When examined at a slit lamp, note that multiple infiltrates, merging with each other, form a pattern resembling a branch with leaves. This type of keratitis is considered superficial and is called “tree-like.” In prognostic terms, it is more benevolent than another type of herpetic lesion of the cornea - discoid keratitis.
With this disease, the infiltrate is round and quite intense due to inflammatory processes occurring deep in the stroma. A characteristic feature of such inflammation is its long course; sometimes the doctor and the patient do not notice the positive results of treatment for a long time.
Another common viral keratitis is adenoviral. As an independent disease, it does not occur; it always accompanies the course of adenoviral conjunctivitis and other manifestations of adenoviral infection. Upon examination, small infiltrates are detected in the corneal epithelium. They dissolve for quite a long time. In particularly advanced cases and with improper treatment, they can leave behind cloudiness and significantly reduce vision.
Among endogenous keratitis, inflammation of the cornea due to syphilis and tuberculosis is noted. Considering that the basic treatment of these specific diseases is currently at a fairly high level, these keratitis are very rare.