In the 90s, the cornea was examined with an ultrasound “pencil”. Instead of a full map of the cornea, there were 10-15 measurements per eye, from which the surgeon formed a mental picture of what the patient had there. In 1992, topographers based on the Placido system became widespread. The idea is that if you make a projection of light rings onto the cornea, then on an ideal one they will be round, and any distortion will result in a distortion from the circle. That is, such a target was obtained in the eye in an ideal case, and an egg in case of astigmatism. That's how they looked - they shone a beam through Placido's disk. Now many surgeons have such discs in their pockets just in case.
The method was, of course, very approximate. Then automation came: the same disks became 32-36 rings instead of 8 or 10, and the device photographed them, and then recognized and calculated distortions, and produced a “depth map” of the eye.
This is the “target”
"Map of depths" of the eye
At the same time, for diagnosing keratoconus, it was important to measure the cornea not from above, but from the side, and in parallel, the technology of the Orbsken topographer developed. Instead of a reflection profile, there was a beam in a slit lamp (like in a paper scanner), and it made it possible to obtain the optical environment of the cornea, in particular its back side.
Accordingly, they automated it and did something like measuring dozens of slices, and then assembling them into a single map. Like a computed x-ray tomograph, only simpler and in the light.
The next stage of evolution was the principle of Scheimpflug, that is, a rotating beam. As you can guess from the name, it was invented in Germany, and in the same city where Lake and Oculus are located. Today, the embodiment of this principle, the Pentakam device is the most popular diagnostic device for refractive surgery. There is a lot of information - 4 or 5 other devices were combined into one: here is the thickness, the front surface, the back, the depth of the anterior chamber. And this device is still developing and becoming more accurate.
But the Placido system did not die. In the case of complex patients (and such patients are regularly sent to us when they do not know how to treat problems), it supplements information about the condition of the cornea. In this case, the Placido system is good because the topography of the surface after complications allows you to assemble a surface removal map to the ideal “target”, that is, quickly calculate the difference between what is visible and what needs to be done, and then remove the excess tissue with a laser. This is the so-called topoguided operation. An uneven cornea can be brought into more or less decent condition. SuperLASIK operates on approximately the same principle, which is customized for each individual patient every time. Its analogue, femtoLASIK Custom Vue, is a wavefront-guided laser. The idea here is that the wavefront of the eye is measured, and then the excimer laser blows away the necessary parts of the cornea. The method has pros and cons. The disadvantages are related to the fact that some of the distortions come from the lens; with laser correction, nothing can be done with the lens. The lens changes greatly during life, but the cornea remains almost unchanged. He grows all his life. Accordingly, super-correction in this case is enough for a couple of decades of young active life... As a result, the “ideal” profile for the cornea, which is not related to the current profile of the lens, is now much more often used.
And there is also classical OCT (tomography) - it better shows the thickness of the tissue, and it is additionally used for opacities of the cornea that exclude other methods.
So, based on the diagnostic results, a profile is selected. In the case of modern operations, the surgeon builds a profile in the likeness of a master, entering the necessary data. The mathematics for the aspherical lens is done by flashing the laser, then the surgeon chooses from several possible results or simply confirms the operation scheme.
Here is an ultrasonic “pencil”:
The rest of the modern stuff is at the end of the post. In the meantime, important practical things for the operation.
We do not look through the center of the pupil
The next thing we are interested in is the centering of the cornea under the laser.
The surgeon selects a cone for pneumatic auto-grip - there are three sizes for different tasks. For myopia, the smallest one is most often taken; it is placed on the periphery of the cornea. A minimal number of people look through the center of the pupil. Usually our optical axis is slightly shifted towards the nose - this is the Kappa angle. In hypermetropes (people with severe farsightedness, for example), this angle is larger. It gets to the point that sometimes they look at the very edge of the pupil.
To avoid cutting the lens where it is not necessary, it is important to center it along the optical axis. Therefore, the patient himself looks at the flashing LED. But in reality, of course, we do not completely trust the patient here, and we definitely control the capture by the Purkinje reflex. In the sense of a glare, and not a conditioned reaction. This is the highlight that you are familiar with from the “red eye” in flash photography, but it can be compressed almost to a point. This is not the axis itself, but it is located very close to the reflex, so much so that you can take this point as the center of the lens. In difficult cases, sometimes a point is selected between the center of the pupil and this reflex - it all depends on the preliminary diagnosis.
A reference beam is placed at this location and the ablation center is marked. Then the laser turns on. Excimer lasers have a high-speed camera that monitors the micro-movements of the eye and moves the laser in coordination with them. On older models of lasers during operations, if the patient looked to the side, the laser hit the wrong direction. Since about 2005, eye-following systems have been moving with the beam. In the case of FLEX or SMILE, when a femtosecond laser is used, the eye is simply captured in a pneumatic gripper. There is no tracker, but there is a vacuum loss sensor - before the eye is suctioned, the laser turns off.
Correct grip does not always happen. If this is the case, the surgeon performs additional correction by rotation or re-grip. Capture control is done by superimposing two images - from the camera in real time and from calibration before capture. Someday we will have automatic systems that will superimpose two images and capture correctly automatically. Today it depends on the experience of the surgeon.
A study was conducted - compared 36 patients with femptoLASIK and 36 with SMILE - the location of the tissue evacuation zone in the second case was better. Even on the old MEL-80 (the most modern at that time). The excimer laser generally forgives an inexperienced surgeon a lot. But an experienced surgeon can create better centration on the VisuMAX than a conventional excimer can do automatically. Probably, in the future, firmware and a manipulator will appear that will reduce this factor of the surgeon’s experience and skill.
In Istanbul there was once a very complex patient with two decentrations close to strabismus. It was quite difficult with him, since it was necessary to go through the language barrier, but in the end everything worked out. However, if possible, we always recommend choosing a surgeon who speaks the same language as you for complex cases.
Laser hair removal Magic 3.
As mentioned earlier, almost all laser hair removal devices are based on one of 2 methods:
- Destruction of hair melanin through light radiation
-The light heats the hair shaft, due to thermal effects we see the destruction of the hair shaft directly during the procedure. As a result, the hair becomes thinner and lighter, and then stops growing.
2. Destruction of hair follicles
-The light beam destroys the hair follicle, or rather the vessels surrounding it. The bulb stops receiving nutrition and dies; after the procedure, after a few days, the hair falls out. As a rule, a laser device is based on only one of these techniques, these are the so-called mono devices. Now more modern machines are appearing that can combine several techniques. Such a laser platform is the Magic 3 device. This laser uses several wavelengths that can affect both the hair body and the hair follicle.
What is most important when correcting astigmatism?
This is how a person with astigmatism sees the world:
To simplify, what would give a point on the retina in a healthy person, with astigmatism becomes an ellipse or a “figure of eight” at a certain angle. By determining this angle and the relative size of this distortion, it is possible to make lenses for glasses in which the curvature will change nonlinearly in comparison with conventional lenses for myopia or farsightedness. After some time, they learned to make the same contact lenses (it is important to insert them into the eye without rotating), and then to calculate profiles in order to cut such a “contact lens” directly on the cornea or inside it. That is, to solve the general problem of laser vision correction.
Astigmatism is corrected using laser methods very effectively. However, the most difficult part is the comparison of the future profile of the lens and, in fact, the eye. The fact is that if you miss the turn by 10%, the effect will be lost by a third. If you miss by 30%, the effect will completely disappear. As a result, an important part when working with astigmatism is to capture the eye with the vacuum “suction cup” of the laser. This is a matter of the doctor’s experience (fortunately, not necessarily manual, so they do it well almost everywhere). With modern lasers, it is possible to deploy the grip “inside itself” by slightly rotating the patient’s eye—an Indian research center has proven that this is safe to do.
The essence of the method.
So, as was said earlier, the Magic3 laser hair removal method is based on the combination of several wavelengths in one procedure:
- 532 nm - this light pulse length is characteristic of a green spectrum neodymium laser (Nd:YAG+KTP). This laser affects blood vessels and pigment. Therefore, when used during hair removal, this type of laser radiation coagulates the vessels surrounding the hair follicle. After the vessels are coagulated, nutrition stops flowing.
- 808 nm - this wavelength is used in a diode laser. These wavelengths do an excellent job with melanin (a pigment found in our body). Melanin is found not only in the skin, but also in the hair. It is this pigment that is responsible for the color of the hair. The more melanin in the hair, the more effective the hair removal will be. The beam destroys melanin cells, the hair becomes discolored and destroyed. Already during the procedure itself we see some hair thinning after exposure to the laser.
- 1064 nm - this laser pulse length has a maximum penetration depth, which allows you to achieve the effect of permanent hair removal in any part of the body.
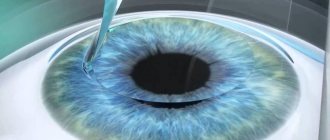
How is a laser focused through lenses of liquid on the surface of the cornea and microdroplets of fat?
When premedication is done with an anesthetic (usually alcaine), quite a lot of drops fall on the surface of the eye. The eye is then wiped at least once with a damp swab immediately before contact with the laser pneumatic gripper. If the eye is dry, gaps will form between the laser cone and the cornea, which will distort focusing. If the eye is wet, the liquid fills them, and there are almost no parasitic refractions. Mirkodroplets of fat are driven away when captured due to pressure. As a result, of course, the resulting environment is still not ideal, and this is partly one of the reasons why the lenticule needs to be “bypassed” with a spatula on both sides, separating it from the upper and lower layers of the cornea. A significant mistake could be this: eyelashes secrete fat, which begins to quickly and uncontrollably spread across the surface. This fat disrupts focusing, and large bridges remain that need to be separated with a sharp spatula (as was done with the previous generation of lasers) - or you need to stop the operation if you see such a problem. In our clinic, we do not leave anything to chance, using a number of necessary manipulations: aspirators to remove excess fluid and fatty droplets, special hygroscopic sponges, we can even deprive you of a pair of eyelashes near the central part of the eye - we will trim them in case they suddenly didn’t bend as much as it should.
Preparing for laser hair removal.
In order for the laser hair removal session to be as effective and comfortable for the patient as possible, it is necessary to properly prepare for the procedure:
- Hair in the treatment area should be no longer than 3 mm.
If the hair is shorter, then the diode laser will also not have much effect, it simply will not recognize the melanin in your hair and will not have the desired destructive effect on the hair. And if the hair is longer than 3 mm, then it is possible to get burns, because... Hair that is too long may melt slightly from the laser beam. The ideal length is 2-3 mm.
- Stop taking photosensitizers.
Photosensitizers are preparations (medicines), ointments and creams containing substances that promote photosensitivity - increasing the body's sensitivity to solar radiation. Typically, manufacturers write on their drugs about this effect. Therefore, if you use any pharmacological drug internally or externally, read its instructions to identify this side effect.
- The intended treatment area must be dry and clean. Therefore, if you come to see a laser hair removal specialist, do not apply any creams, lotions or gels to your skin, especially if it concerns large areas (hips, legs, back, etc.).
What are the most serious complications?
Complications with LASIK are up to 6%, with femtoLASIK and FLEX - up to 2%, with SMILE - 0.5-1% (depending on the generation of lasers, 0.5% is the sixth).
The latest numbers have not been confirmed by ten years of clinical trials - the data will not be officially published until the summer of 2017, but you can look around Wikipedia - articles about different methods provide quite rich links to research. One of the most terrible complications of any correction other than PRK is keratoectasia.
(when the cornea bulges, as in keratoconus). As a result of surgery, this can happen due to a significant violation of the biomechanics of the eye - as a rule, either due to incomplete diagnosis, or due to a surprise that the doctor's diagnostic tools could not detect. That is why it is important to do the diagnosis very carefully and using different methods. It must be admitted that clinics often skimp on the most expensive “reinsurance” equipment. On the other hand, if a patient already comes in with keratoectasia, then he will most likely have a direct indication for good old PRK. In general, any thin cornea, and even one that is not completely smooth, can be smoothed well by PRK. In the early stages of keratotonus, PRK levels the surface and immediately on top we also do cross-linking (treatment with a product high in B12, then the release of oxygen due to laser heating and fixation of collagen in ultraviolet light - everything to make it rigid, but more on that later separately ). This niche will ensure the life of PRK for at least another 10 years.
Keratoconus is a complex complication in the medium term. Cross-linking is done immediately, that is, cartectasis is treated as usual. Intracorneal half-rings can be inserted.
Historically, some of the keratoectasia after SMILE are cases where the surgeon discovered a diseased cornea and decided not to do the invasive procedure LASIK or its derivative, but for some reason decided that ReLEx could “ride” due to its low invasiveness. No. A diseased cornea does not need to be corrected without strengthening. You can do cross-linking, rings, transplantation.
Our next most popular flap is the flap after LASIK, femtoLASIK or FLEX.
More often, of course, they get LASIK - they have a total risk of various side effects of 6%, and at the same time there are a lot of them done in the country even to this day. Any patchwork correction methods are a contraindication for contact sports. You can give birth, but getting punched in the face is undesirable. There were cases when the flap was torn off because a child simply inaccurately poked his finger in his mother’s face, because a woman caught her eye on a tomato stick - in general, all sorts of things. Let me remind you that the essence of the problem is that with these methods a “lid” is cut, which is “folded back” to create a lens inside the cornea, and then this “lid” is closed back. It is connected to the eye by a thin bridge-“loop” and a thin layer of epithelium that has grown on top. The flap does not grow in, and is held in place without opening, only with the help of the superficial epithelium on top. The LASIK flap itself can be removed even after 8-10 years (there have been cases) - and it will come out exactly in the same place as on the day of the operation. In the case of femtoLASIK and FLEX, the flap holds more firmly, there is often scarring along the edges (a thin white stripe) - after 2-3 years you can already try to tear it off with your teeth, and it will not give in. In the case of SMILE, there is no flap at all, but there is a “tunnel” (2.5 mm incision) through which the lenticule is removed from the cornea - it is also covered with epithelium, but before it heals, you cannot wash, so as not to cause an infection. Our colleague from Yekaterinburg talked about a patient with SMILE who was severely beaten - the damage spread across the eye very extensively, but the weakest point was not at the site of correction. The eye was saved and the patient sees well. More precisely, I began to see it after a couple of weeks. A similar case occurred in the practice of Bloom (the second inventor of correction technology). In Germany, to work as a police officer, you can only do PRK in 13 of the 16 federal states. Three more allow femtoLASIK.
Contrary to popular myth, Bowman's membrane, which is located on top of the cornea (which is destroyed during PRK and severely damaged during femtoLASIK methods) does not provide protection against impact-type mechanical damage. It provides “slow” type stability, in particular, it compensates for pressure from inside the eye.
Now it’s worth talking about the halo effect
is a halo around light sources at night. Any laser correction can give it. It depends on the size of the correction zone in relation to the pupil. The usual correction zone is 7 millimeters. Some people's pupils open up to 8 millimeters in complete darkness. Previously, correction zones of 4-5 millimeters were generally made. The second reason for a halo (more relevant to modern surgeries) is how flat your cornea is in the center. The center should be elevated (a healthy cornea has more diopters in the center than at the edges - for example, 38 D in the center, 42 D at the edges). A good professional calculates the profile for laser cutting so that the cornea is flattened over a large area. Excimer lasers have different aspheric profiles for this purpose. ReLEx SMILE itself is aspherical in its very intervention architecture. Yes, the natural state of the cornea worsens with any correction, but with SMILE it is a little less.
Then we have photophobia and tissue overgrowth.
The problem is with the medications. In PRK in Russia, the “usual” metamycin for this operation is not used (it is not approved at the state level). Analogs are a little riskier. Now ophthalmologists are trying to lobby for the approval of this drug for operations.
The next case is incomplete lenticule extraction during SMILE surgery
. There were extremely rare cases when there was a part left that could not be picked up with tweezers. In this case, cortisone is injected, which stains the small fragment and then you can go inside and remove it. In London, one of the very expensive surgeons makes a second cut for such a case opposite the first - he does not use it, but keeps it in case of problems during the operation. Usually, if the laser did not cut something in the lenticule, this is the problem of the surgeon, who for some reason went in and tried to separate the place where there was no cut. That's right - let it heal and do PRK with topography. Or, as an option, switch to FLEX instead of SMILE.
Then tearing the edge of the incision
- a very unlikely thing in experienced hands, when a surgeon with an instrument tears the entrance to the “tunnel” leading to the lenticule. For this to happen in practice, you need to push him in the shoulder during the operation. However, there is usually no problem: the incision was 3 mm, it will become 3.5 mm - no big deal, really. In the vast majority of cases, the incision is torn radially, but there was one example at the very beginning of the history of corrections, when a tear of 1.5 mm occurred towards the center. From a zone of 7.8 mm to a zone of 6.8 mm, the patient received a halo effect in deep darkness. The solution is simple - you need to hold the eye with tweezers with your other hand, since then this has been included in the mandatory SMILE protocol.
Among the serious (but, fortunately, reversible) it is worth noting keratitis
. This is an inflammation of the cornea, most often as a result of an infection. Its three stages - in the second, usually cortisone and treatment at the discretion of the doctor, and in the third, rinsing the pocket is mandatory (there is a risk of irreversible scarring). Therefore, after the operation, you are observed the next day and several more times.
Everything else, as a rule, goes away within a week or two after surgery, and is associated with the body’s reaction to mechanical damage to tissues, or the characteristics of medications. Yes, you may cry for a couple of hours, yes, it may sting, yes, in some people the painkiller then causes a wild desire to touch the eyes (which you should not do). And yes, for the first couple of days it is better for you not to appear at the beauty contest and take portraits for the dating site. Then everything will be fine.
A little history.
Although, if we talk about hair removal in general, then this method of self-care is more than one thousand years old. Even in ancient civilizations it was quite widespread. True, not everyone did hair removal, but mostly rich and noble people. Nefertiti and Cleopatra are known to have used waxing and tweezers to remove unwanted hair. Despite the main disadvantages of these methods, such as pain and short-lived effects, to this day they remain the most popular and used at home, due to their simplicity and accessibility.
Epilation was performed by maids - they spent hours plucking unwanted hairs from the bodies of their housewives. Poor Egyptian women got rid of unwanted hair using sharply sharpened objects. According to historians, these items contributed to the invention of the first razor in Ancient Egypt.
In the cultural society of Ancient Greece, it was considered a disgrace of the highest degree for a woman to have hair in her intimate places. The absence of excess hair (not only on the pubis, but also in other places on the body) was, on the contrary, considered a symbol of female beauty, innocence and youth. Thanks to this, it was the women of Ancient Greece who became the Egyptian heirs to the ideal of smooth skin and beauty.
In Ancient Rome there was also a tradition of getting rid of excess hair on the body. We did this in the bathhouse. Excess hair was removed after the skin was steamed and the pores expanded, which made the procedure easier. The slaves twisted the hairs of their mistress onto a coarse thread and pulled sharply. The ancient Romans used special tweezers and creams, which in their mode of action were reminiscent of modern depilatory creams. They also used epilation with resin (modern waxing). Wax strips were invented in Turkey in the 14th century. They were used to remove body hair from the concubine and wife of Osman the First. And in Turkey, already in the 16th century, bathhouses adopted the presence of special rooms as a standard, where they carried out the removal of unwanted vegetation.
A little later, a method of hair removal using honey and various oils appeared. In the 16th century the first razors appeared, and in the 19th century the first machines appeared.
In Europe during the Middle Ages, excess hair on the body was shaved off, and soft hair was rolled out with bread-wax balls. During the reign of Catherine de Medici, hair removal became an unpopular activity - for some reason, Catherine forbade her close ladies from removing pubic hair. Why she did this, history is silent. When Queen Victoria came to power, hair removal was not done at all.
In the second half of the 20th century, technologies began to develop that made it possible to radically combat hair growth. Electrolysis appears. Initially, the method of destroying the hair follicle using electric current was used in ophthalmology at the end of the 19th century to remove ingrown eyelashes, but it began to be widely used as a tool for hair removal on other parts of the body only in the 70s of the last century. Including in the Soviet Union. The method has a right to exist, but it has enormous disadvantages: burns, pain, a high probability of scarring and low speed of work - about 10 minutes per square centimeter. This method is advisable only in the case of removing gray and pigment-less hair.
My skin is too dark. Will laser hair removal harm me?
Today, laser hair removal is the safest method of permanent hair removal. But it is worth understanding that melanin is found not only in the hair, but also in the skin, therefore, the first laser hair removal devices caused complications in the form of hyper and hypo pigmentation and burns. Today, the Magic3 platform has the ability to perform permanent hair removal even on people with very dark skin, absolutely safely and effectively. The device settings allow you to change not only the length of the light pulse, but also the power, which has a positive effect on the result.
How does a laser hair removal session work?
- Laser hair removal is performed in a cosmetology chair.
- If hair removal is performed on the face, the doctor will first cleanse the skin and remove makeup.
- If the pain threshold is very low, local anesthetic creams can be used. Laser hair removal Magic 3 has a cooling system, so the patient feels very comfortable during the procedure without experiencing pain.
- During the procedure, the doctor may use several laser wavelengths. To achieve maximum effect.
- The time required for hair removal may vary, it all depends on the area of the correction area. On average, it takes about an hour on the legs, while in the area above the upper lip the specialist will need 5-7 minutes.
- After the session, a special regenerating cream is applied to the skin; it will relieve a minor inflammatory reaction and moisturize the skin.
Will I be able to remove blonde hair?
Oddly enough, blonde hair is removed worse with laser hair removal than dark hair. This is due to the ability of the laser to react to melanin; the more melanin in the cell, the more destructive the laser pulse will be for the hair. Blonde hair has less melanin, so a diode laser may not be 100% effective. This is why Magic3 is more preferable as it has different hair removal methods. And if you can’t go down the path of destroying melanin, you can go down the path of destroying the hair follicle by using a different length of the light pulse.