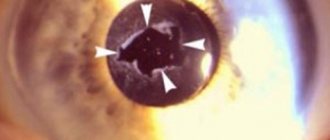
Despite the current progress in cataract surgery, phacoemulsification of intumescent cataracts continues to pose difficulties even for experienced surgeons [1–4]. When opening the anterior capsule of the lens, its uncontrolled linear rupture with divergence of the edges is possible, which in the English literature is defined as the “Argentine flag” syndrome. If this rupture was avoided when opening the anterior capsule of the lens, it may appear during the formation of the anterior capsulorhexis [5-7]. The linear rupture extends beyond the equator and can move to the posterior capsule, leading to prolapse of the vitreous and displacement of the nucleus to the posterior part of the eye [8–11].
To reduce the risk of such complications, the technology of small “controlled” capsulorhexis was proposed in 2003 [5]. In subsequent years, the problem of phacoemulsification of mature intumescent cataracts received further development [9].
The purpose of the work is to improve the technology of phacoemulsification of swelling mature cataracts and to study the mechanism of possible uncontrolled rupture of the anterior capsule when performing anterior capsulorhexis.
Causes of cataracts
Cloudiness of the lens (cataract) can occur at any age and the factors predisposing to the occurrence of cataracts are quite extensive:
- aging of the body
- hereditary predisposition
- eye injuries (concussions, penetrating wounds)
- inflammatory eye diseases
- concomitant eye diseases (glaucoma, high myopia, etc.)
- chemical, ultraviolet, ionizing or radiation effects on the body
- endocrine diseases (diabetes mellitus, hypo- and hyperthyroidism, etc.)
- immune and metabolic disorders, etc.
Age-related changes in the lens
Throughout life, changes occur in the size, shape, consistency and transparency of the lens. In a newborn it is almost spherical in shape, soft, transparent and colorless. With age, the lens takes on the shape of a biconvex lens, with a flatter front surface and becomes yellowish in color, while completely maintaining its transparency. The intensity of the yellow tint increases with age.
The formation of lens fibers occurs throughout life, but the volume of the lens increases only up to a certain age. This is due to the compaction of the central parts of the lens, consisting of older fibers. As a result, the density of the nucleus increases all the time: from a small and soft embryonic nucleus in a newborn, to a clearly differentiated nucleus in an adult (by the age of 25-30), and then large, yellowed and sclerotic in an elderly person.
Around the age of 60, the ability to accommodate is almost completely lost. This is due to compaction and sclerosis of the lens nucleus - phacosclerosis. In this regard, it becomes difficult for a person to clearly distinguish between objects located at a close distance - after 40 years, the so-called presbyopic age begins. During this period, due to a malnutrition of the lens and a slowdown in its metabolism, initial opacities may occur in its various layers.
Symptoms of cataracts
The main symptom of cataracts is blurred vision followed by decreased visual acuity.
But the following symptoms may also occur:
- ghosting
- the appearance of a halo around the light source
- deterioration of color vision
- blurred vision at night
Stages of senile (age-related) cataracts
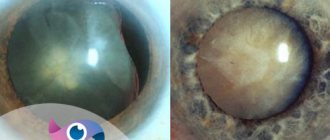
With initial cataracts, clouding of the eye lens appears along the periphery, and the optical zone is transparent. Immature cataract - opacities begin to affect the optical zone. This leads to a noticeable decrease in visual acuity. Mature cataract - clouding occurs throughout the lens. Visual acuity is significantly reduced; only light perception may remain. Overripe cataract - at this stage, the lens fibers disintegrate, the lens substance liquefies and the lens acquires a milky white hue.
All stages of cataracts, except the “initial” ones, require surgical treatment.
Stages of age-related cataracts
The full cycle of disease development can take from several months to several decades. In most cases, the period of initial cataract is the longest, then events develop faster.
Stages of age-related cataracts:
- initial;
- immature;
- mature;
- overripe.
At the initial stage of cataracts, there may be no symptoms of decreased vision; the patient will learn about this from the ophthalmologist at the appointment. In this case, there are minor densities in the lens, usually outside the optical zone.
At the immature stage of age-related cataracts, complaints of visual impairment appear. In myopic patients, the diopter power of glasses increases; they have to be replaced every six months with increasingly stronger ones.
| People with farsightedness, including age-related ones, on the contrary, may notice a paradoxical improvement in near vision and refuse reading glasses. |
This effect is associated with swelling of the lens nucleus and a change in its refraction to a greater extent. This is called “myopization of the cataract.”
During this period, the disease can be classified according to the location of the opacities. They can be located in the cortex of the organ - cortical cataract, the nucleus - nuclear, under the capsule of the lens - anterior or posterior subcapsular.
The immature stage of age-related cataracts is characterized by an objective decrease in vision due to the optical heterogeneity of the lens, but the details of the fundus are determined when examined by an ophthalmologist.
Further progression of the pathology is characterized by the spread of opacities to all layers of the biological lens. At the mature stage of age-related cataracts, visual acuity sharply decreases - down to hundredths. This is called “object vision” - only large objects are visible. When a doctor examines the fundus “behind a thick veil”, it is impossible to examine the optic nerve and retina.
People around may notice a whitish tint to the previously completely black pupil on the patient’s sore eye.
At the stage of overripe cataract, the lens fibers undergo lysis - destruction, until the nucleus descends into the lower parts of the lens bag - “Morgani cataract”.
Similar destructive changes occur in the ligaments that suspend the organ. Overmature cataracts are always complicated.
| In advanced cases, intraocular inflammation may occur due to the penetration of decay products beyond the capsule of the focusing lens. |
Subluxation and dislocation of the lens into the vitreous body - the result of destruction of the zonules of Zinn - also almost always accompanies the final stage of age-related cataracts.
Diagnosis of cataracts
To establish a diagnosis of cataract, it is necessary to conduct a wide ophthalmological examination, including: visometry (determining visual acuity)
- ophthalmometry (measurement of the radii of curvature of the anterior surface of the cornea and its refractive power in different meridians)
- refractometry (determining the optical power of the eye - refraction)
- perimetry (determining peripheral vision)
- tonometry (determination of intraocular pressure)
- biometrics (determining the depth of the anterior chamber, lens thickness, eye length)
- biomicroscopy (examination of tissues and media of the eye using a slit lamp)
- ophthalmoscopy (examination of the fundus of the eye)
These research methods allow you to diagnose the degree of maturity of cataracts, determine concomitant eye diseases, develop treatment tactics, allow you to calculate the strength of the artificial lens when replacing it and determine the prognosis of visual functions in the early and long-term periods after treatment.
Causes of cataract development
Currently, worldwide research into the causes and mechanisms of cataract development (cataractogenesis) is being intensively conducted. This is especially relevant due to the fact that cataracts are one of the main causes of reversible blindness. After all, it is much easier and cheaper to prevent the development of cataracts than to carry out its conservative treatment for years or perform expensive surgical intervention.
The main advances in this area have been achieved in the study of physicochemical processes leading to disruption of the optical properties of the lens. With senile cataracts, changes occur in the chemical composition of the lens. In the initial period of cataract development, the water content increases, the imbalance of a number of ions and amino acids increases, and at the same time the amount of water-soluble proteins and vitamins and ATP decreases. In addition, the activity of a number of enzymes involved in the metabolic process in the lens decreases, oxygen consumption sharply decreases, lipid peroxidation processes, etc. are disrupted.
Currently, there are several theories explaining the occurrence of opacities in the lens. However, each of them separately cannot fully explain the complex mechanisms of cataract development. Most likely, the formation of age-related opacities in the lens is the result of the complex influence of both internal (endogenous) and external (exogenous) factors. Currently, the main cause of cataract formation is the mechanism of free radical oxidation.
Free radicals are chemical compounds that are highly reactive. In the body, they are constantly formed during metabolism, but are destroyed by special enzymes and natural antioxidants. Free radicals are very dangerous - they lead to the destruction of cell membranes and ultimately cause cell death.
In eye tissues, the most significant additional factor stimulating the formation of free radicals is light, especially the short-wavelength part of the spectrum in the range of 200-300 nm. As a result of the formation of free radicals in the lens, toxic compounds are formed and accumulated, leading to irreversible changes in proteins.
A special role is played by the fact that the activity of antioxidant enzymes in the lens decreases with age and the concentration of natural antioxidants (vitamins A, E, glutathione, etc.) decreases.
Prevention and treatment of cataracts
To date, the issue of cataract prevention remains unresolved and causes a lot of controversy.
It is possible to carry out preventive instillations (instillation) into the eyes of drugs that improve metabolic processes and slow down the processes of clouding of the lens substance. Such drugs are prescribed only after an examination by an ophthalmologist.
The only way to treat cataracts is SURGICAL.
The indication for surgical treatment of cataracts is a persistent decrease in visual acuity, limiting the ability to work, causing discomfort and reducing a person’s quality of life.
Now there are several surgical methods for treating cataracts, the most common of which are:
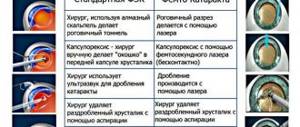
Ultrasound phacoemulsification of cataracts
This method of surgical treatment is currently the “gold standard” of cataract surgery. This operation is performed using an ultrasonic device, the tip of which is inserted into the anterior chamber of the eye through a micro-incision (up to 2.5 mm). After removing the cloudy lens, an elastic intraocular lens (IOL) or, as it is also called, an “artificial lens” is implanted through the same incision in a folded state, unfolding in the capsular bag.
The advantages of the method are:
- painless procedure
- The operation time is less than half an hour
- local drip anesthesia
- no surgical stitches
- minimizing the risk of bleeding and inflammation due to a small incision
- possibility of treatment on an outpatient basis.
extracapsular cataract extraction
This surgical intervention is considered more traumatic and is used in advanced cases of mature cataracts, when ultrasound exposure is not enough to remove the clouded lens.
This method is characterized by a large incision in the cornea and an incision in the anterior capsule of the lens, through which the lens nucleus and its masses are removed from the eye and replaced with an intraocular lens (IOL). The operation ends with suturing, which can lead to postoperative astigmatism.
intracapsular cataract extraction
This type of surgical treatment of cataracts is characterized by the removal of the lens along with its bag, is traumatic and is used extremely rarely, when it is impossible to carry out the first two methods of surgical treatment of cataracts.
In our ophthalmology department, all the necessary preoperative examinations for the treatment of cataracts are performed, and the department’s specialists are proficient in the entire arsenal of surgical interventions.
Phone number to make an appointment or 8
Treatment: Current Issues and Options
The only effective treatment for cataracts is surgical extraction.
with implantation of an intraocular lens. Today, phacoemulsification (destruction of cataracts using the Kelman-Cavitron phacoemulsifier) followed by implantation of an intraocular lens made of acrylic or silicone is one of the most common operations not only in Russia, but also in the world. Phacoemulsification is an expensive but cost-effective intervention: in the USA, the operation costs 3.4 billion dollars per year for 1.5 million people, but over the next 13 years the income reaches 45-67% due to improved quality of life and restoration of ability to work [18].
In Shanghai, the number of cataract extractions from 2006 to 2009 increased from 1741 to 2411 operations per 1 million people [27], from 2006 to 2010 in Iran - from 4723 to 6328 operations per 1 million people [28]. However, at the moment, a decrease in incidence is observed only in a number of Latin American countries, where the frequency of cataract extractions more than doubled between 2005 and 2012 [29]. An increase in cataract surgery is only possible through large government programs such as the “free phacosurgery for a million poor” coupled with updated health insurance policies in China [30, 31] or the World Bank-supported program in India [32]. Lack of access to medical care is a pressing issue: according to a 2012 review, by that time there were 204,909 ophthalmologists practicing in the world, while the growth in the number of specialists in developed countries is half as fast as the increase in the number of people over 60 years of age. In developing countries, there is an even more pronounced shortage of specialists [33]. In former socialist countries and Latin American countries, up to 85% of ophthalmologists are not trained in cataract surgery [29]. Taking this into account, one of the goals of the VISION 2021 initiative put forward by WHO was defined as at least 4 ophthalmologists per 1 million people.
However, even a satisfactory supply of specialists does not guarantee quality medical care [34]. Higher quality medical care is associated with location in an urban area, a physician’s experience of at least 2 years, and work in non-governmental organizations [28]. A partial solution to the problem is the spread of microinvasive cataract extraction, which does not require expensive equipment and causes fewer complications for novice surgeons than phacoemulsification [35].
However, insufficient access to medical care is not always the main cause of vision loss from cataracts. In societies with low education, patients refuse even free surgery, citing rumors about possible blindness after surgery [10, 36]. Also, despite a significant decrease in quality of life due to cataracts, 9 out of 10 patients are not ready for surgical treatment psychologically or for medical reasons [37].
Conservative treatment
Cataracts have not been sufficiently developed and studied at the moment.
Available data focus on drugs that potentially slow the progression of cataracts. A number of clinical studies are devoted to the drug Oftan
®
Katachrom
(Santen Pharmaceutical, Japan; produced in Tampere, Finland). The active ingredients are nicotinamide (vitamin PP), the antioxidant cytochrome C and adenosine, which plays a key role in energy metabolism. Adenosine is a precursor to ATP, which ensures all metabolic processes. Nicotinamide (nicotinic acid amide; vitamin PP) stimulates the synthesis of nicotinamide dinucleotide, which, in turn, is a cofactor for dehydrogenases. Cytochrome C is a heme-containing protein of the cytochrome class with antioxidant function.
According to a placebo-controlled, double-blind, parallel study published in 1987, the combination of these active ingredients statistically significantly inhibits the development of lens opacities over a period of 6 months. [40]. The first study of Oftan® Katahrom eye drops in the domestic literature is the work of G.S. Polunina, published in 2001. 158 patients who received Oftan® Katachrom or azapentacene were selected for the study. In the group of patients receiving Oftan® Katachrom, there was a stabilization or decrease in the optical density of the cortical layers of the lens; 62% of patients from this group with cortical cataracts showed an improvement in visual acuity [41].
O.G. Gusarevich et al. studied the normalizing effect of Oftan® Katahrom on the predisposed development of the disease in vivo
. In OXYS rats, which are a biological model for the development of cataracts and macular degeneration of the retina, the use of the drug ensured a significant absence of signs of progression of cataracts and macular degeneration [42].
In the study by E.V. Egorova, 288 patients were randomized into 4 groups: patients receiving Oftan® Katachrom or azapentacene were divided into subgroups that received or did not receive ultrasound therapy. After 24 months Observations in the tear fluid showed signs of improved metabolic processes (absence of pathological interactions of protein and inorganic components) in 28% of patients receiving Oftan® Katachrom, and in 48.9% of patients receiving Oftan® Katachrom with ultrasound therapy (p <0.05 ). By the end of the observation period of 2 years, more than half of the patients who instilled Oftan® Katachrom maintained their initial visual acuity and no new opacities were observed in the lens. Less pronounced changes were observed in other subgroups [43]. Later E.V. Egorova et al. published another study, also on the effectiveness of Oftan® Katachrom eye drops in combination with ultrasound therapy [44].
In the work of T.N. Lumpova Oftan® Katachrom was used in patients with cataracts occurring together with compensated primary open-angle glaucoma of stages I–II. 67 patients (120 eyes) after regular instillations of the drug noted a subjective improvement in vision; in the long-term period, the majority of patients (54% of eyes) experienced stabilization of the process, and in 13% of cases, visual acuity increased. The author suggests that the drug Oftan® Katachrom can contribute to the partial resorption of existing opacities [45].
Complicated cataract - features and differences
Cataract is an eye disease that most often makes itself felt in old age. The protein base of the lens undergoes specific changes with the development of pathology. As a result, the main optical lens loses its inherent transparency and becomes cloudy, which entails a decrease in visual acuity. The disease disrupts a person’s usual way of life. To restore lost capabilities, the patient consults an ophthalmologist.
Complicated cataract is a severe form of disorder that develops against the background of concomitant diseases. Chronic pathologies complicate the course of cataracts, which requires professional help from specialists. Usually the disease develops in one eye, although in medical practice there are cases of the formation of bilateral type disorders (in two eyes).
Pathology develops in young people and elderly patients. Women suffer from this disease more often than men. Lens clouding is irreversible, the pathology progresses, which can lead to complete blindness in a short period of time. A timely visit to the clinic is the only chance to save your vision.
Classification and causes of the disease
Doctors distinguish complicated cataracts associated with general diseases of the body. In this case, the cause of the disease becomes:
- Hormonal imbalances, disruptions in the endocrine system.
- Disharmonious metabolic processes, vitamin deficiency, intoxication.
- Diabetes mellitus (in this case, complicated cataracts develop quickly and easily affect both eyes). The combination of these diseases occurs in 40% of cases. A clear sign of this type is vision that changes throughout the day.
- Convulsions, failure of water-salt metabolism. Lead to the tetanic form of the disease.
- Neuromuscular lesions of a hereditary nature. They provoke the development of myotonic complicated cataracts, which are characterized by numerous areas of turbidity and shiny particles (cholesterol crystals).
- Dermatological problems (eczema, neurodermatic plaques, scleroderma) and other causes.
Concomitant eye diseases
- Inflammation of the choroid and retina (chorioretinitis). Develops with weakened immunity, against the background of bacterial or viral infections.
- Iridocyclitis. The inflammatory process affects the ciliary body, the iris of the eyeball.
- Dystrophic changes in the iris.
- Glaucoma with increasing intraocular pressure.
- Injuries and damage, cancerous tumors.
Congenital eye anomalies play a great role in the development of the disease. During the examination, the ophthalmologist asks questions to determine your medical history and learns about taking medications. This is due to the fact that certain groups of pharmacological agents can also provoke a complicated form of cataract (corticosteroids, glaucoma drops).
Symptoms
The vast majority of cases of this disease have a posterior capsular form. This is facilitated by the lack of normal epithelial protection of the lens, which makes its contact with toxins pronounced. Symptoms of violations:
- Increasing pressure in the eyes.
- The color of complicated cataracts (ivory), which is associated with a large number of infiltrates.
- The patient begins to see worse; when looking at a light source, halos appear before the eyes.
- The ability to adapt vision to night time mode decreases, dark spots appear before the eyes more often, and “spots” flash.
Incomplete cataracts are also characterized by disturbances in the perception of background colors, unclear vision of the contours of objects, and contrasting combinations.
Signs of cataracts in the early stages
The first signs of cataract are individual for each person, and it is very difficult for the average person to independently determine the development of the disease, but the following pathognomonic symptoms are most often observed:
- decreased night vision and blurred vision,
- flickering, flickering before the eyes of stripes, strokes, “flies”, spots,
- poor tolerance to bright light,
- difficulties with visual work at close range (reading text, sewing),
- double vision, distortion of the objects in question,
- weakness of color perception, decreased contrast sensitivity,
- difficulty in selecting points.
Cataract is an insidious disease, and only a highly qualified specialist can diagnose it. However, many patients do not pay attention to the first signs of cataracts, turning to an ophthalmologist only when severe clouding of the lens occurs and vision is reduced to the level of light perception.
Therefore, if you notice the first symptoms of eye cataracts, do not delay having your vision diagnosed by a competent specialist.