Causes
The omission can be physiological, that is, it can be a consequence of the structural features of the organ of vision. In such cases, it is associated with excess skin folds of the upper eyelid. This type of ptosis is also called false ptosis. This type also develops as a result of strabismus.
The remaining causes of ptosis of the upper eyelid are classified as follows:
- Mechanical is the result of eye injuries, foreign bodies entering it, and surgical interventions.
- Ptosis may result from pathologies of the central nervous system . Causes in neurology: cerebrovascular accidents, multiple sclerosis, peripheral nerve palsies, meningitis, encephalitis, myasthenia gravis, tumors.
- of aponeurotic based on stretching or weakness of the muscle that lifts the upper eyelid. This condition is observed with aging and may be a consequence of eye surgery and trauma.
- Sagging can develop after Dysport , a drug used in cosmetology. The medicine consists of botulinum toxin, which causes muscle weakness. This can lead to drooping eyelids.
Video about the causes of eyelid ptosis after Botox:
This is a classification of acquired ptosis, but it can also be congenital. In such situations, maternal pathologies during pregnancy or heredity are important. In such children, there is insufficient development of the muscle that lifts the upper eyelid, or its complete absence.
What it is?
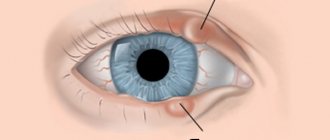
Different pupils: photo
As a rule, the diameter of the pupil of the left and right eyes of an individual person is the same size. The pupil itself is designed to perform the function of regulating the access of light entering the retina.
The human nervous system is responsible for regulating the size of the pupil: for reduction - parasympathetic , for increase - sympathetic . The brightness of the light or its decrease also causes certain muscle groups of the human visual system to work.
With anisocoria, the functions responsible for regulating pupil activity in one of the eyes are disrupted. Physiological anisocoria leads to inconsistency in the work of the muscles of the iris of the visual analyzer. Then in a person, each of the eyes has a different pupil size , which for this reason react differently to the light in the environment.
In people without anomalies of this pupillary function, changes in pupil size are synchronous - when a light signal is received even in one of the eyes, the diameter of the pupils changes in both the left and right eyes. This is exactly how the iris muscles should normally work.
Photo: anisocoria
In nature, anisocoria is considered the norm for many representatives of amphibians or reptiles - their lack of binocular vision (synchronous perception of objects and objects with both eyes at once) causes uncoordinated work of the pupil in each eye.
In humans, the norm is physiological anisocoria with a deviation in the size of the pupils of a pair of eyes of no more than 1 mm in diameter.
Degrees and symptoms
As the name implies, the main symptom is varying degrees of drooping of the upper eyelid. This may result from the fact that the patient is forced to constantly make efforts to lift it. Such actions lead to increased fatigue and emotional lability of patients. They often throw their heads back, especially children.
Drooping of the eyelid interferes with blinking, which leads to dryness and irritation of the mucous membrane of the eye. The tendency to infection of the organ of vision in such cases also increases.
Patients often develop asymmetry of the eyebrows, and children often develop strabismus and the “lazy eye” symptom. Visual acuity decreases, visual fields narrow. Diplopia often develops with ptosis.
There is Marcus-Gunn syndrome , which is also characterized by drooping of the upper eyelid. Its peculiarity is that ptosis disappears as soon as the patient opens his mouth wide or clenches his jaw tightly.
Concomitant symptoms depend on the disease that caused the ptosis. For example, with myasthenia gravis , patients complain of excessive muscle weakness and increased fatigue. With stroke and multiple sclerosis, paresis and paralysis and difficulty walking are noted.
Ptosis can be complete (the eye is completely closed) or partial. The degrees of partial ptosis are as follows:
- Weak is characterized by drooping, in which the eye is open by 5-7 mm.
- With an average degree, the distance is 3-4 mm.
- Severe ptosis is the distance from the upper to the lower eyelid 1-2 mm long.
As already mentioned, ptosis can be acquired or congenital (diagnosed in an infant). It can also be one- or two-sided.
Diagnostics
Diagnosis begins with a history and general examination of the patient. After this, they proceed to a detailed ophthalmological examination. The doctor measures the distance of the palpebral fissure, checks visual acuity and fields, symmetry, and fundus. If necessary, an ultrasound of the eye and an x-ray of the orbit are performed.
Refractometry is required, checking the degree of strabismus, binocular vision, convergence and accommodation. A neurological examination is important. The doctor prescribes electromyography, computed tomography or magnetic resonance imaging for the patient. If necessary, an examination by an infectious disease specialist is carried out.
Treatment options
Treatment can be carried out in different ways. There are surgical and conservative tactics. The choice depends on the causes of ptosis, the characteristics of the pathology in each patient, and the predicted result.
Types of operations
Surgical intervention is indicated in the following cases:
- moderate to severe ptosis;
- complete closure of the eye, a congenital type of disease;
- mechanical damage to the organ of vision;
- the patient's strong desire.
This treatment is usually carried out under local anesthesia.
The most common type of operation is shortening the eyelid, forming a levator duplicator. Excess skin is excised and the edges of the wound are sutured together. To connect them, so-called U-shaped seams are used. This intervention has disadvantages - the sutures may come apart, and the disease in such cases recurs.
Another operation for eyelid ptosis is surgical formation of a duplication of the tarso-orbital fascia . With this type of intervention, in addition to applying U-shaped sutures, cauterization (diathermocoagulation) of the muscles of the overhanging eyelid is also performed. The fold of the eye is strengthened, the level of trauma and scarring is lower, as is the frequency of relapses.
At the present stage of development of ophthalmology, it is possible to strengthen the muscles of the affected eye using a special mersilene mesh , which effectively supports the organ of vision and gives the operated eyelid the most physiological appearance. In such cases, the risk of recurrence is extremely low, but the price of such an operation is higher than previous ones.
Features of treatment in children
Congenital ptosis of the upper eyelid in children almost always requires surgical correction. Operations for children are the same as for adults. The difference is in the anesthesia; for small patients, general anesthesia is required. In the future, physical therapy and constant monitoring by an ophthalmologist are recommended.
What to do with ptosis after Botox
The drooping of the eyelid after Botox on the forehead is associated with an incorrectly calculated dose of the drug, but most often it is a consequence of the individual reaction of the body. Ptosis also develops with pinpoint injections or as a result of disproportionate distribution of the product on the face.
Photo of ptosis of the upper eyelid after Botox
If the overhang is caused by Botox, no specialized treatment is required. Almost always, muscle mobility is restored on its own within 1-2 months.
Treatment of ptosis of the upper eyelid after Botox in such cases is not required. The return of mobility is associated with the removal of the drug from the body.
Sometimes recovery takes 5-6 months. If the process is long, then doctors can prescribe patients a course of physiotherapy and the administration of drugs that improve the transmission of nerve impulses - Proserin, Neuromidin.
Video on how to avoid drooping eyelids after Dysport:
Folk remedies
Some patients have a question about how to get rid of drooping eyelids using traditional medicine methods. Doctors have a negative attitude towards this direction for ptosis, since not a single technique can influence the cause of the disease and eliminate it .
In some cases, the use of traditional methods can only harm the patient (for example, with neurological pathologies). Therefore, if you have such symptoms, it is important to contact a medical facility as soon as possible, rather than carry out treatment at home.
Eliminating ptosis with exercises
Eye exercises are useful for any etiology of the disease. They strengthen muscles and improve their function.
Patients are recommended to blink intensely for 15-20 seconds (6-7 approaches), circular rotations (the head does not move), tightly closed eyes, followed by maximum wide opening. It is also useful to look at the tip of the nose with your head thrown back (duration - 15-20 seconds, after - relaxation of the facial muscles).
It is better to perform these exercises 3-4 times a day for several approaches. This will help achieve better results.
The video clearly shows how to do gymnastics for drooping eyelids:
Physiotherapy
Physiotherapy is aimed at restoring the functional activity of the eye, improving blood flow and metabolism in the affected area. This type of treatment is effective only for neurological etiology of ptosis. In some cases, physiotherapy can have a positive effect on injuries to the organ of vision.
Patients with ptosis are prescribed ultrasound irradiation, myostimulation, electrophoresis, laser and galvanotherapy. Physiotherapy methods do not differ between adults and children.
Stages and classification
In ophthalmology, ptosis is classified according to its causes.
Neurogenic blepharoptosis is formed as a result of systemic diseases. Diabetic neuropathy, aneurysms, and large brain tumors provoke prolapse.
Need advice from a beauty expert?
Get advice from a beauty expert online. Ask your question right now.
ask a free question
Myogenic is formed during myasthenia gravis. The disease is characterized by atrophy of the muscles responsible for small movements. The muscle structures of the tongue, palate, and hands suffer from autoimmune pathology.
Aponeurotic occurs in older people. Ophthalmic injuries lead to it.
Mechanical develops with horizontal shortening of the upper eyelid. Abnormal location is caused by large tumors, scars after injuries, and surgical interventions.
By the nature of its occurrence, ptosis can be congenital, caused by disturbances in the formation of the eye apparatus, which arise under the influence of toxins, radionuclides, ionizing radiation on the body of the mother and child, and acquired - it develops after birth.
Blepharoptosis has three stages of development:
- Partial - lowering to the upper third.
- Incomplete - the edge is located in the middle of the pupil.
- Complete – characterized by complete closure of the eye.
Ophthalmologists determine the severity of the pathology and its stage.
After a detailed interview with the patient and examination, the doctor checks the visual acuity and field of vision.
A final diagnosis requires consultation with a neurologist. The specialist will refute or confirm the neurogenic nature of the disease.
CT and MRI of the brain will help exclude a malignant process.
Prevention
It is important to know what to do to prevent drooping eyelids. When administering Botox, you must follow the optimal dosage of the drug, injection technique, and carefully select injection sites.
Congenital ptosis cannot be prevented. As for acquired forms of the disease, prevention is aimed at eliminating pathologies that can lead to drooping eyelids (as far as possible). Injuries to the organ of vision should be avoided; if ophthalmological or neurological diseases occur, they should be treated promptly and fully.
ICD-10 code
The disease classifier, which has official international status (ICD10), classifies anisocoria in section H57.0 (other diseases of the eye and its adnexa - anomalies of pupillary function), or Q13.2 (congenital anomalies of the anterior segment of the eye - other malformations of the iris).
Modern medical science aims at the existence of 3 groups of pathologies in the synchronous regulation of pupil size:
- congenital or acquired nature, as a consequence of damage to the visual analyzer (eye);
- anomalies in the course of physiological development - anisocoria of a bilateral or unilateral nature;
- anisocoria as a consequence of illnesses experienced by the individual (eye or other kind, but affecting the functionality of the visual organs) or injuries.