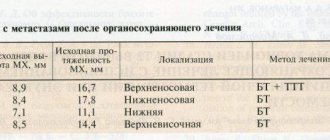
GLAUCOMA is a chronic eye disease in which intraocular pressure (IOP) increases and the optic nerve is affected. At the same time, vision decreases, up to the onset of blindness. Blindness caused by glaucoma is irreversible because the optic nerve dies.
In this case, it is no longer possible to restore sight to a blind patient!
A comprehensive and individual approach to patient management tactics, modern methods of treating glaucoma, offered in our clinic, make it possible to preserve vision and improve the quality of life for patients suffering from this disease.
Today, it has been convincingly proven that the earlier surgical treatment of glaucoma is performed, the more stable and better the patients’ vision is preserved!
Therefore, we successfully use qualitatively new methods of treating glaucoma - effective, safe and low-traumatic surgical operations. Modern high-tech glaucoma surgery is currently divided into: laser treatment of glaucoma and microsurgical treatment of glaucoma.
Laser treatment of glaucoma
Glaucoma surgery has undoubted success, however, it becomes obvious that no matter how great the achievements in the technique of micromanipulation, no matter how small the cutting blade is, even the maximum potential of its capabilities is incommensurate with the task of correcting the pathology of the microstructures of the thinnest filtering zone. eyes. In this regard, the question inevitably arises about searching for ways of “knifeless” microsurgery for glaucoma.
A unique opportunity for this is a laser beam, with which you can perform operations on the membranes and inside the eye without opening its cavity, i.e. without cutting the wall. Laser surgery for glaucoma is performed using a medical laser. The laser beam can be focused into a pinpoint light spot, which plays the role of a “laser needle” or “laser knife”.
LASER TREATMENT OF GLAUCOMA IS PAINLESS, DURABLE AND IS CARRIED OUT ON AN OUTPATIENT BASIS, ALLOWING YOU TO AVOID SURGICAL INTERVENTION ON THE EYEBALL.
Treatment of glaucoma with a laser, unlike surgery, does not require general anesthesia and can be performed on an outpatient basis with a minimum duration of postoperative release from work. Since laser surgery for glaucoma is performed without opening the eye, it is not accompanied by the complications that can arise during and after antiglaucomatous microsurgical operations. Laser treatment of glaucoma has a very significant advantage - restoration of the outflow of intraocular fluid (IOH) through natural channels.
Traction laser surgeries
Currently, laser methods for the treatment of glaucoma are widespread and most effective, the main area of influence of which is the trabecular network of the anterior chamber angle. This laser treatment for glaucoma is called traction laser surgery and consists of applying laser coagulates in the trabecular area, which leads to widening of the trabecular slits and an increase in the outflow of intraocular fluid from the eye.
Today, antiglaucomatous laser operations of this type have proven themselves to be effective for open-angle glaucoma. The most commonly used are the following: linear and radial laser trabeculoplasty, anterior and posterior trabeculospasis, cyclotrabeculospasis .
1 – laser trabeculoplasty
2 – anterior trabeculospasis
3 – posterior trabeculospasis
4 – cyclotrabeculospasis
After laser surgery, it is recommended for some time (up to 2 weeks) to continue taking the antihypertensive drugs that the patient received before the intervention. To reduce the severity of the reactive syndrome and postoperative inflammatory reaction, anti-inflammatory drugs are prescribed locally (in the form of drops). After the symptoms of reactive inflammation disappear, the doses of antihypertensive drugs are gradually reduced or discontinued completely.
OPHTHALMO.RU
From July 18 to July 21, 2007, a world congress was held in Singapore, organized by the Association of International Glaucoma Societies (AIGS).The previous forum, held in Vienna two years ago, brought together various glaucoma societies around the world. It was then that the Russian Glaucoma Society became a member of this organization. Now AIGS ceases to exist, turning into a world-class organization, which will be called the World Glaucoma Association (WOG) and its first forum will be a congress in Boston (USA) in 2009.
The goal of the international organization of glaucoma societies is not only to unite the world's leading resources and the most significant research on the problems of glaucoma, but also to improve the educational level of all glaucomatologists in the world. Another important goal is to achieve consensus on the diagnosis and treatment of glaucoma patients. These problems are solved in the process of international congresses, which for more than ten years have been held in different parts of the globe every two years.
The Congress in Singapore, which attracted about 2 thousand participants, was held at a large exhibition center (Congress Hall Suntec Singapore) with the support and wide participation of leading pharmaceutical companies and medical equipment companies. Ophthalmologists from all over the globe took part in the work. Among the speakers were leading experts from both the USA and European countries. It should be noted that among the congress participants there were a significant number of ophthalmologists from Asian countries.
The day before the opening of the congress on July 17, the US Institute of Graduate Studies organized a symposium “Recent Advances in Neuroprotection in Glaucoma.” The symposium was organized with the support of Allergan.
In his opening remarks, Dr. R. Weinreb (USA) substantiated the need to search for neuroprotective therapy, emphasizing that within 20 years, 27% of patients with glaucoma become blind in one eye and 9% become blind in both eyes, and if, against the background of antihypertensive treatment, patients go blind in 4.4%, then in the absence of treatment - in 9%. Assessing the effectiveness of neuroprotective treatment is a very difficult task, since the result of this type of therapy occurs much later than the immediate effect of local antihypertensive drugs.
Discussing the mechanisms of development of GON, M. Rosarioo Hernadez (USA) paid special attention to the interaction of retinal ganglion cells and glia. Astrocytes, representing the glial tissue of the retina, normally take an active part in the processes of tissue remodeling, replacing dead axons. In glaucoma, astrocytes that produce growth factors and various chemical substances disrupt the normal environment of axons, leading to their death. The trigger mechanism in this case may be directly increased IOP. Along with astrocytes, Müller cells of the retina, also representing glial tissue, regulate the processes of capture of neurotransmitters by retinal ganglion cells, incl. glutamate and regulate ion homeostasis of GCS. The importance of Müller cells in the pathogenesis of GON has been studied much less than astrocytes, which play a key role in the mechanisms of death of axons and RGC bodies.
It is noteworthy that the earliest pathological mechanisms in glaucoma develop in axonal mitochondria and consist in the activation of oxidative stress, structural damage to mitochondria, activation of their enzymes and cell apoptosis. It is believed that it is the mitochondria of RGC axons that are the point of application of early neuroprotective treatment.
An interesting message was given by Dr. N. Gupta (Canada), who emphasized that glaucoma is a neurodegenerative disease not only of the optic nerve, but of the entire visual analyzer. Postmortem studies of the brains of glaucoma patients have revealed changes in the chiasm, lateral geniculate body, optic radiation, and even in the visual cortex. The author concludes that at the moment when patients with glaucoma show changes in the visual fields, reducing the light sensitivity of the retina by half, there are already lesions in the central nervous system (CNS). Dr. N. Gupta's report generated heated discussions. As a result of the discussion, the participants came to the conclusion that soon it will be possible to diagnose glaucoma based on changes identified in the central nervous system (for example, during magnetic resonance imaging). An interesting question is whether the primary lesion in glaucoma is the death of neurons in the visual cortex or in the retina. A debate has also flared up on this issue. N. Gupta believes that the primary lesion is the central nervous system, but we are not yet able to prove this.
Many reports at this meeting were devoted to assessing the rate of progression of glaucomatous optic neuropathy (GON). Indeed, this is not an easy task. It turns out that when assessing the progression of GON using the perimetric MD index, we are convinced that this rate is 0.9 dB per year, and only in 10% of cases is it more than 1.5 dB per year. According to A. Heijl (Sweden), with an initial MD index of -4.0 dB over five years, the index deteriorates to -20 dB only in a fifth of patients. The rate of progression is twice as high in pseudoexfoliation glaucoma. It is noteworthy that local antihypertensive treatment, as a rule, is more effective in reducing IOP, but has a much less effect on the level of change in the MD index. The conclusion from these observations is simple - glaucoma progresses despite normalization of IOP, and the most important factor in progression is the existing glaucomatous lesion (the lower the initial MD index, the faster the progression). In all cases of rapid progression of GON, it is recommended to perform perimetry every three to four months.
What are the real neuroprotectors that we currently have? It is noteworthy that only two of them were mentioned at this symposium, and only one is currently used in practice. We are talking about the α2-adrenergic agonist brimonidine. Scientists from the USA (Wheeler L., Hare W.) have shown that the influx of calcium ions into the cell is successfully suppressed by brimonidine. C. Girkin (USA) in his study on corticosteroid culture demonstrated the protective function of brimonidine, which increases cell survival under conditions of transient ischemia
The glutamate-calcium cascade is also blocked by memantine. This is another neuroprotector discussed extensively at this symposium. Both drugs (brimonidine and memantine) act in a dose-dependent manner and are currently the most promising neuroprotectors.
Considering the prospects for the use of the NMDA receptor blocker memantine, Dr. A. Lipton (USA), emphasized that in recent years huge amounts of money have been spent on researching various NMDA receptor blockers in the treatment of GON, but none of them have been successful due to extreme toxicity of the drugs used. It is important to note that Dr. A. Lipton is a leading neuroscientist in the world who has made major contributions to the development of treatments for neurodegenerative diseases, in particular Alzheimer's disease. His research, especially in the field of the use of memantine in diseases of the central nervous system, was awarded high awards in the USA. A. Lipton drew the attention of ophthalmologists that to obtain a neuroprotective effect in GON, very small doses of memantine are required (which ones are not yet known!). An overdose will lead to the opposite effect - to the activation of NMDA receptors. That is why today this drug is not approved in the United States for use in glaucoma, but remains one of the most promising in the future neuroprotective treatment of GON.
Let us remember that the goal of glaucoma treatment, according to the recommendations of the European Glaucoma Society and international standards, is to maintain the quality of life of patients for as long as possible. This implies not only the preservation of visual functions (their level is assessed mainly by the ability to drive a car), but also takes into account economic and social aspects, i.e. at what cost is this preservation of visual fields achieved? It should be emphasized that an entire symposium was devoted to issues of quality of life, at which ophthalmologists came to the conclusion that quality of life with glaucoma suffers much earlier than was previously believed. Dr. A. Viswanathan (Great Britain) emphasized that this occurs between the transition of glaucoma from the initial stage to the advanced stage: 71% of patients already in the initial stage of the disease experience problems associated with driving a car. Dr. R. Hitchings (Great Britain) proposed to assess the quality of life of patients with glaucoma, namely, to determine their ability to drive a car, to evaluate the integral visual fields, i.e. results of overlaying perimetry data from both eyes. They showed how much more informatively such an approach reflects the level of damage to visual functions.
Interestingly, neuroprotective treatment, according to most speakers, is more indicated for patients with so-called IOP-independent glaucoma. In other words, if the progression of GON has little to do with high IOP, and more with other, for example, vascular factors, then neuroprotective treatment will be the leading therapeutic method. It can sometimes be difficult to differentiate these patients. But apparently, this determines the more or less benign course of GON in different patients: if there is a certain mechanical factor in the deflection of the sclera latticework membrane, which can be eliminated by reducing IOP, then the progression of GON can be stopped. It’s another matter when GON is determined by other factors, for example, vascular dysregulation, then neuroprotective treatment enters the arena, in which the world’s scientific ophthalmologists, as summarized at the end of the symposium, have not yet been very successful.
The work of the congress itself, which began the next day, was structured on the principle of combining plenary sessions in large conference rooms with thematic symposia-courses, which were repeated at different times so that participants could attend as many events as possible that interested them. What was new in the organization of the congress was the holding of so-called debates, a list of which was sent out long before the start of the congress, so that participants could decide on the most interesting topics. During the debate, leading experts discussed some problem (for example, normal-tension glaucoma or what's new in glaucoma surgery, as well as glaucoma as a neurodegenerative disease, etc.) among themselves and with those present in the hall. During the debate, a consensus was developed.
A significant number of reports were devoted to angle-closure glaucoma (ACG), which is not surprising, because It is this form of glaucoma that occurs most often in Asia, where the congress actually took place. According to H. Quigley (USA), this form of glaucoma leads to disability to a greater extent than POAG. Among the 60 million patients with glaucoma on the globe, 44 million have an open-angle form, and 16 million have a closed-angle form, and the latter is especially common in China (five times more often than in other regions of the globe).
The meeting devoted to the pathogenesis of various forms of glaucoma was very eventful. Dwelling on the mechanisms of development of PACG, Dr. D. Lam (Hong Kong) drew the attention of ophthalmologists to a common cause of increasing retention with a closed angle in the form of adhesion of the iris root to the pigmented part of the trabeculae. The formation of goniosynechia leads to long-term and even permanent retention, which ultimately affects the condition of the optic nerve. Some comments were made regarding terminology: acute angle-closure glaucoma is understood as a condition corresponding to an attack, and chronic is understood as a disease in which glaucomatous optic neuropathy occurs as a result of constant narrowing or closure of the ACP.
Considering the mechanisms of development of angle-closure glaucoma, R. Ritch (USA) focused on four main ways of formation of retention: pupillary block, flat iris, closure of the APC by the lens and malignant glaucoma. The author emphasized the importance of gonioscopy, which allows one to differentiate the functional block from the organic one (there are synechiae). Particular attention is paid to the shape of the PGR with a flat iris. The diagnosis in this case is most accurately made according to ultrasound biomicroscopy, when a small posterior chamber is detected, which, in principle, is not typical for PACG. In this case, the presenters strongly recommended performing peripheral iridoplasty.
Much attention was paid to modern methods of visualizing the anterior segment of the eye using OCT. At the same time, dwelling in more detail on the assessment of the state of the CPC, D. Friedman (USA), drew attention to the disadvantages of each of the existing methods: even the most informative of them, OCT, does not allow visualization of the ciliary body, which is extremely necessary for choosing tactics for managing a patient with ZUG. It is important to remember that only 20% of patients with a closed angle develop an attack of glaucoma, while the rest develop chronic glaucoma. Quigley H emphasizes that only one in 10 patients with a narrow UPU develops PAAG. An important role in this, according to the author, is played by the condition of the vitreous body and choroid.
In the pathogenesis of POAG, Dr. E. Tamm (Germany) paid special attention to the deposition of extracellular matrix in the juxtacanalicular part of the trabeculae. The cause of this phenomenon is considered to be excessive synthesis of transforming growth factor (TGF β 2).
Talking about the pathogenesis of pigmentary glaucoma, Dr. R. Ritch (USA), emphasized that this is a hereditary disease, transmitted in an autosomal dominant manner, and associated with damage to the metabolism of seratonin, dopamine and tyrosine. The disease manifests itself mainly in the third decade of life and declines as presbyopia progresses, because the greatest release of pigment from the pigment layer of the iris occurs during accommodation. Treatment of pigmentary glaucoma, according to the speaker, should be genetic.
Dwelling in detail on the mechanisms of development of pseudoexfoliative glaucoma (PEG), Dr. U. Schlotzer - Schrehardt (Germany), emphasized that the disease is a manifestation of stress-induced elastosis and elasto-microfibrillopathy, the key points of which are excessive synthesis of TGF β 1, oxidative stress and mild inflammatory process. The speaker drew attention to the systemic nature of the disease and emphasized the role of impaired ocular perfusion during PEG. It was noted that the disease is especially common among emigrants from Russia (epidemiology is not represented in Russia itself).
In the pathogenesis of normotensive glaucoma (NTG), according to M. Wax (USA), much remains unclear. It is assumed that the mechanisms that damage the retina and optic nerve in NTG may be based on both hereditary causes and disruptions of normal physiological processes due to the following predisposing factors: 1.vasospasm, 2.vascular dysregulation, 3.morphological disorders of the sclera such as, for example, with myopia, 4.formation of anti-phospholipid antibodies, 5.genetic damage, 6.aponoeia during sleep, 7.autoimmune mechanisms. During the discussion on the problems of IGT, the need for frequent IOP measurements was repeatedly emphasized, especially at night, when there are peaks in the rise of IOP. Dr. Yamomoto noted that in Japan there is a practice of measuring IOP and blood pressure when examining patients with normotensive glaucoma every four hours during the day. Doctors from Europe for IGT focus on measuring ocular hemodynamics, which is widely practiced in Germany and Switzerland.
Several sessions were devoted to discussing the role of IOP in the development and progression of glaucoma. This emphasizes the fact that our foreign colleagues attach great importance to IOP in the pathogenesis of the disease, but still call it a risk factor. At this congress, at least several important statements were made regarding the role of intraocular tone in the development of glaucoma. Firstly, the importance of 24-hour tonometry was emphasized, especially at night, since measuring IOP in the first half of the day is low informative. It should be noted that foreign ophthalmologists recognize the leading role of high IOP in the progression of GON. However, the role of diurnal IOP fluctuations in disease progression is no longer recognized as a significant risk factor. If recently they talked about a high correlation between the level of IOP and the thickness of the cornea in its central part, it is now emphasized that there is no direct correspondence between these concepts, and measuring the thickness of the cornea is most important from the point of view of the risk of progression of GON (the thinner the cornea, the higher this risk). Finally, a very important summary was made regarding target pressure. It is recommended that when calculating this indicator, it is based on the stage of glaucomatous damage, on the expected remaining life expectancy for a particular patient (for this purpose, graphs for recalculating the current age for the remaining years have even been demonstrated!), as well as associated risk factors, including the condition of the fellow eye and family history on glaucoma. Risk factors for the progression of GON (by the way, they are also risk factors for the transition of ocular hypertension to glaucoma), studied in several multicenter studies, were summarized at this symposium. Among them, it should be noted high IOP, thin cornea, large excavation of the optic disc (vertical), asymmetry of the optic disc between the two eyes, high perimetric PSD index, age, low perfusion pressure, migraine, hemorrhages on the optic disc, pseudoexfoliation syndrome, pigment dispersion syndrome and several antiglaucoma history of operations. It is noteworthy that diabetes mellitus, myopia and IOP fluctuations are currently not considered as serious risk factors and their role in the development of the disease remains to be clarified.
Important importance at this congress was given to the assessment of structural and functional changes in determining the rate of progression of glaucoma. Analyzing the literature since 2003 on functional tests for glaucoma, D. Garway-Heath (UK), emphasized that standard automated perimetry (SAP), which is most often used in the diagnosis of glaucoma, is unacceptable for early detection of the disease. For this purpose, the most appropriate use of blue-yellow perimetry (SWAP) or frequency-doubled perimetry (FDT). However, an analysis of the literature has shown that it is difficult to identify the advantages of one of these selective methods of functional diagnostics. The ideal of them can be considered the one that has high reproducibility, allows you to identify early disorders of photosensitivity and, most importantly, is easy to perform and easily tolerated by the patient.
Emphasizing the importance of studying structural changes in glaucoma, L. Zangwill (USA) was based on the provisions developed by AIGS: 1. Methods of structural studies in glaucoma should be included in the routine practice of an ophthalmologist, 2. Color stereo photography of the optic disc is the most important method for assessing the state of the optic disc in glaucoma. 3.Additional methods using digital technology and accompanying database are very useful in assessing disease progression. 4. The use of several computer methods for assessing structural changes in the optic disc and the retinal nerve fiber layer (RNFL) allows the most accurate assessment of the stage of the disease.
An interesting study was carried out by ophthalmologists in India who studied the effect of physical exercise (including yoga) on IOP. It turned out that moderate physical activity significantly reduces ophthalmotonus. However, when doing yoga in the head position, as well as when lifting weights, as well as athletic exercises, IOP rises. A short-term increase in ophthalmotonus is observed during mental stress. The authors recommend taking into account the results obtained and recommending that patients with glaucoma use local antihypertensive drugs when playing sports, for example, instilling pilocarpine for pigmentary glaucoma.
Many reports have been devoted to the molecular mechanisms of the pathogenesis of glaucoma. The reports on gene therapy were of particular interest. Dr. T. Borras (USA) reported on the results of identifying genes responsible for the processes of physiology and pathophysiology of the trabecular meshwork, as well as methods for delivering gene preparations directly to the trabecular zone using an adenoviral vector. Among the identified genes were caldesmon, tropomyosin (genes responsible for the formation of the drainage zone), calcification processes (osteoglycin, matrix-Gla), proteins that protect against stress (myocillin, αβ-coistallin) and signaling neuropeptides (substance P, secretogranin). Interestingly, the search for gene drugs is moving towards drugs that increase the outflow of intraocular fluid. The advantages of gene therapy are its greater efficiency and significantly lower toxicity compared to traditional treatment, which is due to the selective effect of gene drugs.
If the first two days of the congress were devoted to the problems of epidemiology, diagnosis and pathogenesis of various forms of glaucoma, then the next two days were devoted to the problems of treatment. In particular, much attention was paid to the choice of patient management tactics. Obviously, it is individual in nature, but it is fundamentally important to decide where to begin treatment of newly diagnosed glaucoma: with the prescription of drops, or with laser treatment? Opinions on this matter are divided. Proponents of laser treatment as the first stage of therapy referred to the great effectiveness of this method: the patient does not miss instillation of drops, because in some cases he simply no longer needs them. However, argon laser trabeculoplasty causes scarring of the APC structures. This was the main argument of supporters of drug treatment. Against this opinion, an argument was put forward that the modern type of trabeculoplasty, SLT, is a very gentle and at the same time effective method. However, in developed countries, treatment of glaucoma traditionally begins with the prescription of local antihypertensive instillations, and, as a rule, we are talking about monotherapy. At the same time, it was noted that after two years, 49-75% of patients need to be prescribed additional drops, and then it is worth seriously thinking about prescribing fixed combinations of drugs. Such drugs as Cosopt, Combigan (unfortunately, these drugs are still not available in our country), Xalacom, etc. Several posts were dedicated to this. Proponents of prescribing fixed combinations of drugs claim that they produce fewer side effects (apparently due to a decrease in the concentration of the preservative benzalkonium). However, it can be more difficult to establish which component of the combination used is effective and which is not.
A major challenge is the treatment of glaucoma in developing countries. In the report “The Role of Cyclodestruction in the Treatment of Glaucoma in the Third World,” H. Quigley expressed doubt that diode cyclocoagulation can solve the problem where surgery is not available. The author emphasizes that although performing diode cyclocoagulation does not require high technology, nevertheless, studies of the long-term consequences of this procedure in third world countries are very limited and the results of these studies are not very reassuring (only in two thirds of cases it is possible to achieve a reduction in IOP to 22 mm Hg And this is after several procedures). As an alternative measure, the author suggests performing laser trabeculoplasty. As for diode cyclocoagulation, this method is more indicated for patients with refractory glaucoma.
Comparing the effectiveness of two methods of laser trabeculoplasty - argon and selective, R. Ritch emphasized that they are both equally effective, with the only difference that SLT is more effective in elderly patients and can be repeated, this is its advantage, however, the results of SLT in secondary glaucoma remains to be studied. The author emphasized the low effectiveness of laser trabeculoplasty in young patients, especially with high myopia.
The question of the advisability of performing peripheral laser iridectomy with a closed anterior chamber angle is still controversial. Dr. Thomas (India) outlined the consensus on this issue: the procedure is indicated in all cases of an attack of angle-closure glaucoma, incl. and to prevent an attack on the fellow eye. At the same time, it is known that about 8% of the population have a narrow or closed UPC (which manifests itself in goniscopy, when the UPC is closed 180 degrees when performing specific tests). However, this condition is benign in most cases and progresses to chronic angle-closure glaucoma within five years in only 22% of cases, usually without leading to blindness. Therefore, the indications for prophylactic iridectomy in such cases are relative. It is more important, according to the author, to identify risk factors for the development of PAH in time and take timely measures.
At the video session on surgery, much attention was paid to combined surgery, and the authors repeatedly emphasized that the choice of tactics for sequential or simultaneous cataract and glaucoma surgery in all cases is decided individually. Such details of surgical technique were considered as the choice of IOL for phacotrabeculectomy, preservation of conjunctival and scleral flaps, implantation of IOL for ruptures of the posterior capsule and zonular ligaments, as well as for a narrow pupil. It should be emphasized that great attention is still paid abroad to the use of antimetabolites (mainly mitomycin C) in the prevention of excessive scarring. More than one meeting was devoted to the choice of doses and technique for using MMS. Khaw (UK) noted the advantages of the punch technique in performing sinustrabeculectomy, emphasizing the lower risk of postoperative hypotension. At the same time, the author insisted on tight suturing of the scleral flap. The discussion of what to do in case of unsuccessful antiglaucoma surgery was interesting. The question of whether to perform a revision of the previous zone, perform anti-glaucoma surgery in a new place, or switch to laser cyclodestruction periodically arises before any glaucoma surgeon. Dr. A. Manda (Canada) believes that preference in this case should be given to surgery in a new place, using MMC or drainage. Laser cyclodestruction is indicated for low visual functions of the patient.
Summing up the results of the last forum, it should be noted that the emphasis of the ongoing research, including promising ones, is on the neuroprotective treatment of glaucoma. That is why the most important of these studies (in particular, in the field of memantine and adenoviral vector drug delivery) have received awards and worldwide recognition. The modest participation of Russian ophthalmologists in the development of world glaucomatology is regrettable.
The report was prepared by Professor N.I. Kurysheva
Transscleral laser cyclocoagulation
In this case, laser treatment of glaucoma consists of thermal destruction of part of the ciliary body in order to reduce the production of aqueous humor and intraocular pressure.
Indications for this laser treatment method:
- primary glaucoma in an advanced stage, not amenable to traditional treatment methods,
- terminal glaucoma with pain syndrome that cannot be controlled by traditional methods of treatment,
- vascular ophthalmic hypertension and glaucoma, regardless of the stage of the process (post-thrombotic after acute obstruction of the central retinal vein, neovascular after acute occlusion of the central retinal artery, hemorrhagic after recurrent hemophthalmos),
- diabetic neovascular degenerative glaucoma,
- post-traumatic glaucoma and ophthalmic hypertension (including post-burn).
Patient preparation and stages of laser cyclocoagulation of the eyes
Before performing the manipulation in question, the doctor conducts a visual examination of the patient and also prescribes a set of diagnostic measures:
- Checking visual acuity.
- Computer refractometry to identify factors that provoked visual impairment.
- Biomicroscopy allows you to assess the condition of the components of the eyeball.
- Ophthalmoscopy. Provides an opportunity to study the eyeball from the inside; test the structure of the optic nerve head.
- Non-contact tonometry for daily IOP measurement. Before surgery, the patient is prescribed medications that help normalize intraocular pressure.
- Examination using an ultrasound machine and optical tomography are additional diagnostic methods that can be prescribed in individual cases.
A couple of days before laser cyclocoagulation, the patient’s general health is checked, which includes:
- General blood and urine analysis.
- Biochemical blood testing.
- ECG.
The operation algorithm is as follows:
- Local anesthesia. Lidocaine injections are often used. The anesthetic takes effect within 7-10 minutes.
- Application of laser coagulates to the area where the sclera meets the cornea.
Most often, the choice is made in favor of the transscleral method. It is simple and minimally invasive, but there is a high probability of damage to nearby tissues. The transpupillary imaging method is used slightly less frequently. The operator can dose the effect on the ciliary processes, ensuring high effectiveness of the procedure. However, this technique is fraught with a high risk of developing exacerbations in the future. Another method of performing laser cyclocoagulation is endoscopic. With its help, the surgeon is able to fully monitor the progress of the operation. Due to technical complexity, this method is not widespread today. - The laser is set with an initial power of 1750 mW and a duration of 2 seconds. If after the specified period there is no click (“pop”) from inside the eye, the power is increased. After the “pop” is heard, the power is reduced each time by 250 mW until the specific sound disappears completely. The distance between laser coagulates is about 2 mm.
If repeated surgery is required, it is carried out no earlier than 3-4 weeks after the first laser cyclocoagulation.
Laser iridectomy (iridotomy)
| Indications for laser iridectomy are the same as for surgical ones. Laser iridectomy is used for primary and secondary angle-closure glaucoma, and mixed glaucoma. Laser iridectomy is indicated as an additional intervention after intraocular surgery for incomplete excision of the iris or closure of its coloboma with adhesions and pigment. For prophylactic purposes, laser iridectomy can be performed on the second eye with primary unilateral angle-closure glaucoma and as a preliminary step before trabeculoplasty in eyes with open-angle glaucoma and a narrow anterior chamber angle. Laser iridectomy is contraindicated in cases of corneal edema and opacities and in cases of shallow anterior chamber. |
Laser transscleral cyclophotocoagulation for glaucoma. Price in Moscow
Cyclophotocoagulation , also called cyclotherapy or cycloexcision by specialists, is a widely used method for treating complex eye diseases. The method is prescribed in the case of a blind eye, with constant pain syndrome and in the final terminal stage of glaucoma.
Transscleral cyclophotocoagulation is considered the last argument of the ophthalmologist if other methods of combating the disease do not bring the desired effect, and it is not possible to use the necessary groups of drugs and we are talking about the safety of the eye.
The essence of the transscleral cyclophotocoagulation method
The main goal of the cyclophotocoagulation procedure is to reduce the volume of fluid in the eye cavity. This is achieved surgically, with partial destruction of the ciliary body that produces moisture.
In the recent past, when ophthalmic lasers were only a dream of specialized clinics, they tried to treat the ciliary body using electrodiathermy (electrotherapy) or cryotherapy sessions. True, such attempts had a weak therapeutic effect and did not allow controlling the volume of artificially destroyed tissue.
Often, such destructive effects of the above procedures led to undesirable consequences when the normal functioning of the eye was jeopardized due to the loss of the required amount of moisture.
Unlike previous options, transscleral cyclophotocoagulation is a much more accurate minimally invasive method. At the same time, it is carried out practically without complications - destruction and infection of the tissues undergoing the operation.
Such positive aspects of the cyclophotocoagulation procedure are the reason why it is prescribed to patients with high IOP levels. After all, this category of patients often experience severe pain, leading to damage to the optic nerve and complete loss of visual functions.
Types and types of cyclophotocoagulation
Modern ophthalmology can offer a number of methods that make it possible to establish the production of the required volume of intraocular fluid. At the same time, the cyclodestruction procedure is usually divided into separate methods:
- Cyclocryotherapy, a method of exposure to liquid nitrogen, used quite rarely;
- Contact transcleral cyclophotocoagulation, when a semiconductor G-probe of a contact laser is used for exposure;
- Non-contact transscleral cyclophotocoagulation, which uses a neodymium YAG laser;
- Endoscopic cyclophotocoagulation.
The option of endoscopic cyclodestruction, or endocyclofotocation, is often preferable to other methods. It can be performed as a stand-alone procedure or combined with cataract surgery.
The procedure involves inserting a special probe into the eye, equipped with a microlaser with a light source. By moving the probe around the iris, the ophthalmologist assesses the condition of the ciliary body. This is followed by laser exposure, after which the liquid is produced only by the remaining part of the ciliary body cells.
To perform the operation, both diode and neodymium lasers are used.
Indications and contraindications for cyclophotocoagulation
Indications for transscleral cyclophotocoagulation surgery are the following diseases and eye conditions:
- Terminal stage of any type of open-angle glaucoma (neovascular, traumatic, primary and secondary).
- Consequences of unsuccessful keratoplasty.
- Painful blind eye.
Contraindications to the procedure include severe manifestations of uveitis, malignant neoplasms in the distal part of the eye, and normal visual acuity.
Peripheral iridoplasty and puppilloplasty
Iridoplasty (gonioplasty, iridoretraction) involves applying light laser coagulates to the periphery of the iris. Wrinkling and retraction of the iris stroma leads to an immediate widening of the anterior chamber angle. The operation is indicated for closed-angle glaucoma in cases where iridectomy is impossible or ineffective, as well as for open-angle glaucoma with a narrow anterior chamber angle profile as a preliminary step for subsequent trabeculoplasty.
Laser pupilloplasty is indicated in cases of angle-closure glaucoma when iridectomy cannot be performed. 20-30 coagulates are applied to the pupillary zone of the iris in one of its sectors in several rows. The contraction of the iris stroma is accompanied by a tightening of the pupil in the same direction and a release of the anterior chamber angle in the opposite direction.
Laser treatment of glaucoma, performed on time and according to indications, is a highly effective method of glaucoma surgery.
Laser treatment of glaucoma is effective in more than 90% of cases at the initial stage of open-angle glaucoma; at an advanced stage of glaucoma, the positive result of treatment decreases to 83%, and at advanced and terminal stages it is only 52% and 34% of cases, respectively. A decrease in effectiveness in primary open-angle glaucoma as the disease progresses requires surgical treatment, moreover, laser surgery is ineffective in juvenile glaucoma and primary glaucoma in young people.
Laser treatment methods
About 10 generally accepted methods of laser therapy for glaucoma have been developed. The most widely used technologies are cyclocoagulation, iridectomy, trabeculoplasty, non-penetrating sclerectomy, carried out using a laser.
Cyclocoagulation
Laser cyclocoagulation makes it possible to achieve a reduction in intraocular pressure in glaucoma, even in the case of acute forms of the disease. Thanks to it, it is possible to prevent the onset of complications: glaucomocyclic crises, optic neuropathy, uveitis.
The processes of the ciliary body are involved in the production of intraocular fluid. During cyclocoagulation, they are cauterized with a laser beam. This leads to decreased fluid production and decreased pressure inside the eyeball.
Micropulse cyclocoagulation reduces intraocular pressure by at least 80% of the initial value and is more often used for acute glaucoma. Another type of procedure, transscleral diode laser coagulation, is more preferable for chronic cases. Both methods are recommended to prevent complications in the late postoperative period.
Deep non-penetrating sclerectomy
This is an effective but complex technique that requires highly qualified physicians. It is called non-penetrating because the anterior chamber of the eye is not affected. The Schlemm canal is opened without knife penetration. In this way, it is possible to create an additional path for the outflow of intraocular fluid.
Iridectomy
Laser iridectomy is most often indicated for angle-closure glaucoma. During the operation, a laser makes a small hole through the iris. It serves as a kind of drainage. This helps normalize the pressure between the chambers of the eye.
Iridectomy prevents attacks of angle-closure glaucoma, the transition of the acute form of the disease to chronic. It also helps remove iris adhesions.
Trabeculoplasty
Laser trabeculoplasty is the most common non-invasive laser procedure used for glaucoma. During its course, the patency of the channels of the trabecular network of the eye, through which the intraocular fluid is filtered, is restored.
Two types of procedures are used: argon laser (ALT) and selective (SLT). The second type of operation is more preferable, since it uses a low-temperature laser. The SLT procedure can be repeated 4 to 6 times, and ALT - no more than 1 time.