The appearance of a congestive optic disc (OPND) is associated with swelling of local tissues, which occurs against the background of diseases of the meninges and adjacent structures. In this case, the main cause of the development of the disorder is considered to be intracranial hypertension, which causes headaches and other severe symptoms. Due to swelling of the optic nerve fibers, the retinal vessels are sharply dilated.
If a congestive optic disc is detected, treatment is aimed at reducing intraocular pressure, for which medications are used.
The structure of the optic nerve and the course of the disease
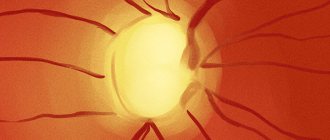
The optic disc is pale pink. With swelling, the color of these tissues changes. Deviations of the optic disc in ophthalmology are diagnosed using a special device (ophthalmoscope).
The optic nerve runs from the disc to the meninges. It is these fibers that transmit information about what a person sees. Next, the incoming data is processed by the subcortical part of the brain, and then by the occipital lobe.
Depending on its location, the optic nerve is divided into several parts:
- intraocular;
- intraorbital;
- intratubular;
- intracranial.
All parts of the optic nerve converge in the bony canal. Here the tissues enter the brain. The normal size of the optic nerve head is 3 cm.
The nature of the symptoms caused by swelling of the optic disc is determined by the localization of the pathological process. Moreover, in all cases, due to the pressure experienced by the disc tissue during hypertension, the quality of vision decreases.
ZDZN is unilateral or bilateral in nature. That is, the tissue of the optic nerve extending from one or both eyes swells. The first option is characterized by mild symptoms. With bilateral edema, the pathological process progresses rapidly: the first signs of visual impairment are observed after several hours or days.
Reasons for the development of edema
Regardless of the characteristics of the symptoms of congestive optic disc, the causes of the development of the pathological process are due to increased intracranial pressure. It develops due to an imbalance of fluids in the skull. Due to the accumulation of cerebrospinal fluid in the area of the optic nerve, disc atrophy develops over time, leading to the onset of complete blindness.
Possible causes of the development of perineural papilledema include brain diseases:
- benign and malignant tumors;
- intracranial bleeding;
- traumatic brain injury;
- suppuration of tissues inside the skull;
- cerebral edema;
- accumulation of cerebrospinal fluid inside the skull (hydrocephalus);
- craniosynostosis (congenital pathology);
- improper fusion of skull tissues (after injuries or due to birth trauma).
Brain infections that cause meningitis and encephalitis lead to optic disc congestion. Also, ZDND is often diagnosed against the background of the following pathologies:
- renal failure;
- hypertension;
- stroke;
- lymphoma;
- sarcoidosis;
- leukemia
The risk group for developing optic nerve edema includes people with diseases of the organs of vision. Often, PVD develops against the background of glaucoma.
One of the causes of disc edema is inflammation of the optic nerve. This pathology occurs against the background of various diseases, including atherosclerosis. Nerve fibers become inflamed due to impaired blood microcirculation. Toxic poisoning of the body causes similar consequences. Moreover, the most dangerous is the influence of ethanol.
Prevention
To prevent the development of atrophy, first of all, it is necessary to promptly treat all ophthalmological diseases. To do this, at the first signs of decreased vision, you need to contact an ophthalmologist.
In addition, it is important to adhere to the following rules:
- Treat infectious and other diseases in a timely manner.
- Avoid injuries, especially traumatic brain injuries.
- Undergo preventive examinations with an ophthalmologist.
- Stop drinking alcohol, quit smoking.
- Be active in sports, particularly swimming.
- Do not read or practice activities that require visual concentration in poor lighting.
- Try to avoid a position where the bright sun shines directly in your face.
- Do not sit in front of the monitor or other gadgets continuously.
- If your eyes are tired, you can wash them with cold tea.
Stages of development of congestive optic disc
The development of papilledema goes through 5 stages, although some researchers distinguish 3 stages. This gradation is based on the nature of the changes that have occurred in the structure of intracranial tissues.
Perineural edema develops during the following stages:
- initial;
- expressed;
- pronounced;
- preterminal;
- terminal.
Congestion of the optic discs at the initial stage is characterized by minor damage. The tissues located above and below swell first. Then the pathological process spreads to the nasal side. Over time, the swelling covers the entire area of the disc, including the vascular infundibulum. At this stage of development, there is a slight expansion of the veins.
At the second stage, disc prominence occurs, which is characterized by an increase in its size. At this stage, the arteries narrow and the veins dilate. At a pronounced stage, the boundaries of the disc are blurred. Minor hemorrhages in the retina are also possible due to disruption of the integrity of the capillaries.
As the pathological process progresses, the intensity of the general symptoms of stagnation increases.
During this period, the size of the disc increases greatly compared to the norm. Local tissues turn red due to impaired outflow of venous blood. The vessels are practically not visible through an ophthalmoscope due to the proliferation of the disc. The number of hemorrhages at a pronounced stage increases.
This stage is characterized by the appearance of whitish lesions in the structure of the eye. The symptom occurs against the background of the onset of tissue degeneration.
Having reached the preterminal stage, the pathological process causes atrophy of the optic nerve. The disc takes on a grayish tint. Swelling at this stage decreases. At the same time, hemorrhages and white lesions disappear. Edema tissues are localized mainly along the borders of the disc.
At the terminal stage, optic nerve atrophy restarts, causing decoloration. The optic disc becomes pale gray, and its boundaries lose their previous outline. The number of arteries in the last stage decreases, but the number and condition of veins remains practically unchanged. Overgrowth of glial and connective tissues is possible.
By secret
- Incredible... You can cure your eyes without surgery!
- This time.
- No trips to the doctors!
- That's two.
- In less than a month!
- That's three.
Follow the link and find out how our subscribers do it!
Source: aokulist.ru
Congestive optic disc
- This non-inflammatory swelling of the optic nerve occurs when intracranial pressure increases.
Etiology
: The development of a congestive optic disc is caused by brain space-occupying formations (tumors, hematomas, abscesses and vascular aneurysms), processes that disrupt the circulation of cerebrospinal fluid (hydrocephalus, thrombosis of the cerebral sinuses, meningitis, encephalitis, spinal cord tumors and uremia); brain injuries, kidney disease, hypertension; in young children, hydrocephalus and birth trauma can cause the development of a stagnant disc.
As a result of increased cerebrospinal fluid pressure, compression of the nerve fibers of the optic nerve occurs. Axoplasmic stasis occurs, which leads to papilledema. The level of increased intracranial pressure largely determines the severity of papilledema.
Clinic
: In most patients the process is bilateral. Subjective manifestations, including decreased visual acuity, usually do not occur before the onset of optic nerve atrophy. Patients complain of headaches, and sometimes there may be short-term blurred vision.
Ophthalmoscopic picture
in the initial stage, blurring of the upper and lower borders of the optic nerve head is revealed. Gradually the swelling increases and spreads to the nasal and temporal halves. At the stage of developed edema, the optic disc is enlarged, the surface of the disc becomes pale and rises above the level of the surrounding retina (mushroom-shaped protrusion of the disc into the vitreous body), its edges are blurred, the veins are sharply dilated, tortuous, and the arteries are narrowed. There are multiple hemorrhages on the disc and in the adjacent retina. With a stagnant disc, visual functions persist for a long time. Long-term congestion of the optic disc eventually leads to the development of secondary optic atrophy with complete loss of vision.
Treatment
is aimed at eliminating the cause of the congestive disc (removal of brain tumors, treatment of meningitis, arachnoiditis, cerebral hemorrhages, etc.).
During the examination of the patient and before the operation, dehydration therapy is carried out, which helps reduce pressure on the nerve fibers of the optic nerve and prevents their atrophy. Prescribe IV glucose solution daily, calcium chloride solution daily; IM - magnesium sulfate solution, furosemide solution 2 ml once every 2 days. Diacarb is given internally. Dexamethasone solution is administered retrobulbarly.
Optic atrophy
(replacement of nerve fibers with connective tissue) - occurs as a result of damage to the axons of the optic nerve and is a consequence of various pathological processes.
Classification of optic nerve atrophy:
According to the state of the disk boundaries
: primary, or simple atrophy of the optic nerve (the boundaries of the disc are clear), and secondary (post-inflammatory or post-congestive) atrophy of the optic nerve (the boundaries of the disc are blurred).
According to the degree of preservation of functions
: partial and complete.
According to the dynamics of the pathological process
: stationary and progressive.
By location of the lesion
: one-sided and two-sided.
Etiology
:
- circulatory disorders;
- compression of the optic nerve in the orbit, in the optic canal or in the cranial cavity (tumors, brain abscesses, aneurysms, hematomas, skull fractures, encephalitis);
- toxic effects (tobacco toxins, methanol, isoniazid, ethambutol, alcohol poisoning, quinine poisoning);
- metabolic disorders (for example, diabetes mellitus);
— traumatic injuries (in particular, contusions);
- degenerative processes in the retina, accompanied by the death of ganglion cells;
— optic neuritis (papillitis);
- congestive optic disc.
— multiple sclerosis, syphilis, blood diseases, hypertension, vitamin deficiencies, atherosclerosis,
Clinic
: Patients complain of decreased vision up to blindness, changes in color perception, and impaired peripheral vision.
Ophthalmoscopic picture
: narrowing of retinal vessels, blanching of part or all of the optic nerve head.
Diagnostics
perimetry (using white and colored objects), craniography (with a mandatory targeted image of the sella turcica of the skull), electrophysiological and fluorescein angiographic studies.
Treatment
use vitamin therapy, vasodilators, nootropic and antisclerotic agents; ultrasound therapy, magnetic, laser and electrical stimulation of the optic nerve.
• To improve the trophism of the optic nerve, retrobulbar prescription is given: atropine sulfate solution, dexamethasone solution, prednisolone solution, fibrinolysin (1000 units) in combination with heparin (500 units), 8-10 injections per course of treatment; solutions of papaverine hydrochloride, trental, complamin.
• IV solution of aminophylline, solution of glucose with ascorbic acid.
• IM solutions of no-shpa, dibazole, complamin, trental.
• IM vitamins B, B2, B6; lidase; cerebrolysin; phosphadene solution.
• Vitreous humor is injected subcutaneously; biogenic stimulants (aloe extract, FBS, etc.).
• Halidor, nicotinic acid, nikoshpan, glutamic acid, riboxin, prozerin, trental, nootropil, cavinton are prescribed internally.
• Ultrasound on the open eye (treatment is more effective in the initial stage of atrophy development); endonasal electrophoresis of no-shpa.
Source: StudFiles.net
A congestive nipple is a non-inflammatory swelling of the optic nerve, most often associated with increased intracranial pressure. Currently, the term “congestive nipple” is being replaced by the more general and more relevant term “papilledema”. The swelling is not limited to one disc, but also extends to the optic nerve trunk. As a rule, a congestive nipple is a bilateral lesion, often equally expressed in both eyes. In rare cases it may be one-sided.
Papilledema is not an independent disease, but a symptom of various pathological processes. In the majority of patients (up to 90%), the cause of the development of a congestive nipple is diseases of the central nervous system, mainly brain tumors. In addition, a congestive nipple can develop with various pseudotumors (tuberculomas, gummas, cysts, parasitic cysts), as well as with encephalitis, meningitis, meningoencephalitis, arachnoiditis, hydrocephalus, and skull injuries. It is observed in general diseases of the body - diseases of the kidneys, blood (lymphogranulomatosis, leukemia, red blood cells, etc.), hypertension, helminthic infestation, Quincke's edema. Diseases of the eyes and orbit are the cause of the development of a congestive nipple in 1.2-4.6% of patients. In children, the occurrence of a congestive optic nerve nipple is most often associated with skull deformations of various origins (“tower” skull), hydrocephalus, neuroinfections, birth trauma, and brain tumors.
An edematous disc in children can occur quite early (within 2-8 weeks from the onset of the underlying disease). This refutes the point of view of some researchers, according to which, due to non-fusion of cranial sutures at an early age, the intracranial process can occur without edematous discs.
The pathogenesis of papilledema has not been definitively established . The most recognized at present is the retention theory proposed in 1912 by K. Behr, according to which a congestive nipple is a consequence of retention of tissue fluid that normally flows into the cranial cavity. According to modern concepts, edema with increased intracranial pressure is the result of impaired microcirculation in the optic nerve and changes in the circulation of tissue fluid in the perineural slits. When intraocular pressure decreases (for example, with eye injuries, etc.), swelling is caused by a change in fluid flow in the optic nerve (instead of centropetal to centrifugal), i.e., in the direction from the brain.
With the long-term existence of edema, proliferation of glial elements occurs and inflammatory phenomena develop due to irritation of tissue elements by edematous fluid. Subsequently, as the process progresses, gradual death of nerve fibers and their replacement with glial tissue is observed, and optic nerve atrophy develops, which is both ascending and descending.
The clinical picture of a congestive nipple is varied and dynamic, it depends on the nature and localization of the process. Conventionally, five stages are distinguished: initial, pronounced, pronounced (far advanced), preterminal (edema with transition to atrophy) and terminal.
Initial stage . The first signs of a congestive nipple are blurring of its borders and marginal swelling, expressed in mild prominence. Initially, the edema affects the upper and lower edges, then the nasal side and much later - the temporal edge of the disc, which remains free from edema for a long time. Gradually, the swelling spreads to the entire disc, last of all involving the area of the vascular funnel. The retina around the disc has mild radial striations due to edematous impregnation of the layer of nerve fibers. There is some dilatation of the veins without tortuosity.
The pronounced stage is characterized by a further increase in the size of the disc, its prominence and blurred boundaries. The veins are dilated and tortuous, the arteries are somewhat narrowed. In some places, the vessels seem to drown in the edematous tissue. Hemorrhages may appear in the marginal zone of the disc and around it due to venous stagnation, compression of the veins and rupture of small vessels. White foci of extravasation often form in the edematous disc tissue.
In a pronounced (far advanced) stage, stagnation increases. The distance of the disc above the level of the retina can reach 6.0-7.0 diopters, i.e. 2-2.5 mm. The diameter of the disk increases sharply. The hyperemia of the disc is so pronounced that its color almost does not differ from the background of the surrounding fundus. The vessels on the disc are poorly visible, as they are covered with edematous tissue. On its surface, various hemorrhages and white spots are visible, which are the result of degeneration of nerve fibers. Sometimes (in 3-5% of patients) whitish lesions can appear peripapillary and even in the macular area, forming a star or half-star figure, as in renal retinopathy (pseudoalbuminuric neuroretinitis).
In the preterminal stage, with prolonged edema, signs of optic nerve atrophy begin to appear. First, a light but clearly defined grayish tint of the disc appears. The swelling begins to decrease, the width of the veins returns to normal, and the arteries narrow somewhat. Hemorrhages resolve, white spots disappear. The disc becomes off-white, slightly enlarged in size, and its boundaries are unclear. In some cases, slight swelling remains along the periphery of the atrophic disc for a long time. Secondary atrophy of the optic nerve gradually develops (terminal stage of atrophy). The disk becomes white, its boundaries remain not entirely clear. The phenomena of secondary atrophy can persist for a very long time, sometimes several years, but ultimately the boundaries of the disc become quite distinct and a picture of primary atrophy appears.
The dynamics of development of a congestive optic nerve nipple may vary by stage and largely depend on the nature of the underlying disease. Sometimes the transition period from initial to pronounced edema takes only 1-2 weeks, in other cases the initial stage can last several months. If the cause of a congestive nipple is eliminated even before the development of secondary atrophy, then all signs of edema regress and the fundus of the eye can normalize. Papilledema can have an intermittent course, disappearing (until complete normalization of the fundus) and reappearing.
A congestive nipple is characterized by the preservation of normal visual functions, both visual acuity and visual field, for a long period (several months, sometimes more than a year). During the period of preserved visual functions, attacks of short-term decrease in vision, sometimes sharp, to light perception, can be observed. At the end of the attack, visual acuity is restored. These attacks are associated with fluctuations in intracranial pressure, when, with a sudden increase in pressure, the force of pressure on the intracranial segment of the optic nerve increases and the conduction of nerve fibers stops.
Subsequently, central vision decreases gradually, the rate of its decline depends on the degree of progression of the underlying process. Usually there is a certain parallelism between the ophthalmoscopic picture and the state of visual acuity. As the edematous disc enters the atrophy stage, vision decreases more rapidly. Sometimes at this stage the patient becomes blind within 1-2 weeks. An edematous disc is characterized by an early expansion of the boundaries of the blind spot, which can increase 4-5 times. The field of vision remains normal for a long time; its developing narrowing is associated with the death of nerve fibers.
Hemianoptic defects and central scotomas are observed in the so-called complicated congestive nipple, when the underlying process (brain tumors, parasitic cysts, inflammation) has a direct or indirect effect on one or another part of the optic nerve or visual pathway, causing a corresponding dysfunction. Complicated congestive nipple is characterized by: 1) atypical changes in the visual field; 2) high visual acuity with a sharply changed field of vision; 3) a significant difference in the visual acuity of both eyes; 4) a possible sharp decrease in visual acuity without atrophic changes in the optic nerve or against the background of initial, mild atrophy; 5) development of atrophy of the optic nerve in one eye with bilateral edema, etc. In children, a complicated congestive nipple often develops with skull deformities of various origins.
The diagnosis of congestive optic nipple is established on the basis of anamnesis (headache, nausea, periodic blurred vision), a characteristic ophthalmoscopic picture of bilateral lesions, the results of a study of visual functions, laboratory and instrumental studies (x-ray of the skull and orbits, calimetry of retinal vessels, measurement of systolic and diastolic pressure in retinal arteries, fluorescein angiography, etc.) and general examination of the patient.
In the initial stages, a congestive nipple must be differentiated from optic neuritis. In this case, one should take into account the marginal edema characteristic of a congestive nipple and its glassy nature, the preservation of visual functions for a long period, and bilateral damage. Electrophysiological parameters (electroretinogram, electrical sensitivity and lability of the optic nerve, evoked potentials) with congestive nipple are normal. The narrowing of the arteries and dilatation of the veins, as well as an increase in diastolic and systolic pressure in the retinal arteries, revealed by calimetry are among the early symptoms of increased intracranial pressure and papilledema. The blind spot, increasing with stagnant disc, remains normal with neuritis.
Sometimes the ophthalmoscopic picture of retrobulbar neuritis, due to the presence of collateral edema, may be similar to that of a congestive nipple. However, a rapid decrease in vision, central scotoma, and more often observed unilateral lesions indicate the presence of an inflammatory process.
The stability of the ophthalmoscopic picture and visual functions with pseudoneuritis and drusen makes it possible to distinguish them from a congestive nipple.
Treatment of a congestive nipple consists of treating the underlying disease. The prognosis depends on the nature of the underlying disease and the effectiveness of its treatment.
- < Back
- Forward >
Source: glazamed.ru
Symptoms of the disease
During the first 6 months after the onset of edema, the pathological process is asymptomatic. In rare cases, glare spots appear. It is also possible that vision and color perception may temporarily become blurred, and the silhouettes of people and objects become blurred. At the same time, symptoms characteristic of increased intracranial pressure are concerning:
- headaches, the intensity of which occurs during coughing, in the morning or during other stress;
- attacks of nausea that develop into vomiting;
- double vision or flickering in the eyes.
Symptoms of papilledema at the initial stage of development of optic disc disease are diagnosed during an ophthalmological examination, which shows the presence of minor hemorrhages on the retina around the disc. The reaction to light remains unchanged.
The appearance of a congestive optic nerve nipple is noted at the stage when atrophy of local tissues develops. This causes blind spots (scotomas). In advanced cases, the patient stops seeing large sectors. In addition, loss of peripheral vision is possible.
Diet
Diet for eyes, nutrition to improve vision
- Efficacy: therapeutic effect after 2 months
- Timing: constantly
- Cost of products: 1800-1900 rubles. in Week
, it is necessary to consume foods that help strengthen tissues and saturate the body with protein , vitamins B6 and B12 , A , D. The following products are recommended:
- fresh milk, cream, sour cream, cottage cheese, cheeses;
- eggs;
- Fish and seafood:
- chicken, rabbit, liver;
- seeds, nuts, flax seeds;
- vegetables, greens;
- cereals;
- legumes;
- honey;
- fruits, berries.
Diagnostics
If signs of congestive optic disc disease occur, you should consult an ophthalmologist. Without timely treatment, the pathological process causes blindness in one or both eyes.
Diagnosis of optic nerve disc disease is carried out using an ophthalmoscope.
The device allows you to examine the condition of the fundus and identify swollen tissue. Before the procedure begins, special drops are injected into the organs of vision to dilate the pupil. After this, a directed beam of light is applied to the retina of the eye.
To differentiate congestive optic disc from brain diseases, MRI and CT are used. If necessary, a cerebrospinal fluid examination is performed to determine the causes of the development of spinal disc disease. In some cases, a biopsy of brain tissue is used.
General information
Optic nerve atrophy is degenerative changes in the optic nerve that appear as a result of pathological processes developing from the retina to the lateral geniculate body. During the process of atrophy, the fibers of the optic nerve gradually die, and information from the retina to the brain is transmitted in a distorted form. Atrophy of the optic nerve can be associated with various reasons, most of which are caused by ophthalmological diseases. Optic nerve atrophy, ICD-10 code H47.2, can be either a congenital or acquired process. This is a serious disease that, without timely treatment, can lead to vision loss. This article will discuss the symptoms, causes and treatment features of this pathology.
Methods for treating edema
The basis for the treatment of congestive optic disc consists of procedures whose action is aimed at eliminating the root cause of the development of the pathological process. In particular, techniques are used to eliminate increased intracranial pressure. For this purpose, the treatment regimen for papilledema is often supplemented with surgical intervention.
Surgeries are performed if cerebral palsy is caused by brain tumors of any nature. During the procedure, overgrown tissue is excised. Also, as part of surgery, a hole is sometimes drilled in the skull, which temporarily normalizes the pressure.
For swelling of the optic nerve, corticosteroids are indicated: Methylprednisolone or Prednisolone. To stop the pathological process, hormonal drugs are used in the form of tablets or solutions.
To eliminate stagnation of cerebrospinal fluid inside the skull, diuretics are prescribed: Furosemide, Acetazolamide and others. These drugs are also used as tablets or as an intravenous solution. With the help of diuretic drugs, the removal of excess fluid from the body is accelerated, due to which swelling disappears.
In case of infection of brain tissue, broad- or narrow-spectrum antibacterial drugs are used. In addition to these medications, antihistamines are used to eliminate swelling.
In case of congestive optic disc disease, dietary nutrition aimed at reducing body weight is recommended. This approach often helps reduce intracranial pressure and provide relief to the patient.
In advanced cases, fenestration of the optic nerve sheath (shunting) is performed. In this procedure, the surgeon creates holes in the tissue surrounding the disc through which excess fluid can drain. Several shunts are also installed to divert cerebrospinal fluid from the spinal cord towards the abdominal cavity.
This type of surgery is mainly used for benign tumors in the skull.
Preventive measures
It is quite difficult to prevent the appearance of papilledema, since the pathological process develops against the background of diseases and disorders, including those that a person is not able to prevent. To prevent congestion in the brain, it is recommended to prevent the activity of bacterial microflora and parasites, regardless of the location of the latter.
When treating inflammatory pathologies, it is recommended to strictly follow medical prescriptions and avoid overdose of medications. This is especially true when antibacterial medications are used. It is also important not to interrupt treatment ahead of schedule, even if the symptoms of the disease do not bother you for several days.
For early diagnosis of edema, it is recommended to undergo an ophthalmological examination every 6 or 12 months. The disease occurs suddenly and in the initial stages of development does not provoke pronounced symptoms.
Despite the fact that there are no specific methods for preventing this disorder, the measures described above help reduce the risks of developing DLD.
The pathology develops against the background of increased intracranial pressure, which is caused by infections, inflammatory and other ailments. In case of PVD, the use of corticosteroids and diuretics is indicated. In advanced cases, the deviation is treated with surgery by shunting the affected optic nerves.
Treatment with folk remedies
Folk remedies can be used in the treatment of optic nerve atrophy only as auxiliary methods. You should consult your doctor before using any of them. Traditional methods will help stimulate metabolic processes, improve blood circulation and relieve inflammation.
- Decoction of cones. You need to mix 100 unripe pine cones, 1 sliced lemon, 25 g rue flowers. Pour everything into 2.5 liters of water, add 100 g of sugar and cook for half an hour. Drink 1 tbsp three times a day before meals. l. The reception lasts for a month.
- Mallow and burdock . Grind the roots of these plants, take 3 tbsp. l. each, add 1.6 liters of water and cook for half an hour. After this, add 4 tbsp to the container. l. collecting herbs. It includes: 2 parts each of sweet clover herb and lemon balm leaves, 1 part spring primrose. Cook for another 10 minutes, then strain. Drink 1 tbsp. l. three times a day for a month. Repeat the course in two weeks.
- Blueberry . It is recommended to eat blueberries every day, as well as prepare a blueberry decoction. This berry contains the pigment anthocyanoside , which is important for the eyes, as well as a number of vitamins. You can prepare blueberries with sugar in the summer by grinding them in a 1:1 ratio. Store this mixture in the refrigerator, consuming 50 g every day.
- Carrot and beet juice. Every day you should prepare a mixture of these juices or drink them separately. It is important that they are fresh.
- Hemostatic herbs. Decoctions should be prepared from them if the patient has hemorrhages in the eyes. These are knotweed grass, stinging nettle, horsetail, and viburnum bark.
- Gymnastics to improve vision. There are also special eye exercises to help improve visual acuity. However, they should never be performed without the approval of a doctor.