Optic nerve glioma is a common ophthalmological disease and is characterized by a pathological proliferation of astrocytes, the supporting cells of the nervous system. This disease can develop at any age, but most often occurs in children under 10 years of age. The pathology is mainly diagnosed in females. Optic nerve glioma is characterized by gradual progression and mild symptoms. Treatment is most often done with a combination of surgery and radiation therapy.
What it is?
Optic nerve glioma is a primary benign neoplasm that develops from the optic nerve trunk. This type of eye tumor accounts for 1/3 of all oncological processes in the visual organs. The pathology is characterized by an infiltrative growth pattern, does not affect the dura mater and can be located in any part of the optic nerve. Sometimes the tumor even goes deep into the skull.
The disease most often develops in children aged 5-10 years, although recently cases of glioma in adult patients over 20 years of age have increased significantly.
Often the disease occurs simultaneously with Recklinghausen's neurofibromatosis.
Causes
At the base of the optic nerve are axons surrounded by glial cells, which produce myelin, promote metabolism, and maintain the functioning of the nerve. From these cells, optic nerve glioma originates, which then grows into the surrounding membranes and spaces, moving along the nerve trunk. As the tumor grows, it increases in size and can reach the size of a chicken egg. The functions of the eye gradually become impaired, up to the complete loss of visual functions.
The exact reasons for the development of such a pathological process are still unknown. Most experts believe that glioma occurs against the background of grade I neurofibromatosis, a hereditary predisposition to cancer.
Disease prognosis
The prognosis for optic nerve glioma depends on the location of the tumor.
- Intraorbital forms give positive dynamics after treatment.
- Intracranial position and glioma of the decussation region lead to death in half of the cases due to the difficulty of surgical access to the tumor.
The prognosis for maintaining visual function is absolutely unfavorable.
Delayed radiation complications are possible in children when exposed to radiation. When the impact on the body is minimized, the quality of life does not suffer.
Consequences of improper treatment
Errors happen in medicine. Sometimes they are committed by doctors, sometimes by patients themselves, using unauthorized folk remedies or untested drugs.
The consequences of self-medication or an incorrect medical approach (long diagnosis, incorrect diagnosis) lead to a complete loss of visual function and subsequently death.
The tumor is located next to the brain, and often, spreading to it, causes lesions:
- optical paths;
- other nerves;
- the brain itself.
The consequence of this is loss of vision, and sometimes death.
Classification of pathology
Based on the structure of the tumor tissue, optic nerve glioma can be of several types:
- astrocytoma – develops from astrocytes, occurs most often;
- ependymoma - arises from epithelial cells;
- oligodendroglioma – forms in brain tissue;
- Brain stem glioma – localized in the stem part of the central nervous system.
In adults, meningioma, a tumor growing from the cells of the arachnoid mater, can be diagnosed. There are also mixed gliomas, which consist of several types of cells. Taking into account the location of the tumor, 2 types of disease are distinguished:
- intraorbital – the tumor is localized in the cranial area;
- intracranial – the tumor is located in the orbital area;
- chiasmal glioma – pathology occurs in the area of the optic chiasm;
- intracerebral glioma – a tumor grows in the brain tissue.
In addition to true gliomas that arise as a result of the proliferation of glial tissue, gliomatosis is encountered in ophthalmology, a pathological process characterized by an increase in the size of glial cells.
Symptoms
At the initial stage of development of the disease, there are no pronounced clinical manifestations; the only manifestation is visual impairment. This symptom usually goes unnoticed in young children, and at an older age it is often mistaken for progressive myopia. As the tumor grows, the symptoms become more pronounced, the following signs appear:
- exophthalmos (protrusion of the eyeball);
- strabismus;
- keratitis;
- scotoma;
- restriction of eyeball movement;
- inability to close eyelids;
- drying of the cornea;
- keratitis, corneal ulcers.
Optic nerve glioma is accompanied by progressive and irreversible vision loss. Cysts often form in the tumor cavity, and an increase in the degree of hyperopia is also observed. If a glioma of the chiasm and optic nerves is formed, the following symptoms are observed:
- decreased visual acuity in both eyes;
- developmental delay;
- nystagmus;
- endocrinological disorders.
Read in a separate article: Congestive optic disc: causes, symptoms and treatment
You can also suspect the development of a benign neoplasm in the visual structures based on the following signs:
- sleep disturbance;
- nausea, vomiting;
- frequent migraines;
- lethargy;
- loss of appetite;
- pain behind the eyeballs;
- memory impairment;
- excessively protruding veins on the head.
When a tumor develops intracerebrally, symptoms depend on which part of the brain is affected. The most common types of ataxia, hydrocephalus and sensory disturbances are observed.
Optic nerve tumors
- Meningioma
- Glioma
- Diagnostic methods
- Treatment
Primary tumors of the optic nerve, despite their benign nature, inevitably grow into the cranial cavity and cause not only blindness, but also the death of the patient.
Neurogenic tumors are derivatives of a single germinal layer of the neurozctoderm and, according to summary statistics, account for 20-30% of orbital tumors.
- Tumors of the optic nerve are represented by two groups: meningiomas and gliomas.
- Tumors of peripheral nerves, depending on the source of development, are divided into neuromas (schwannomas) and neurofibromas (plexiform, diffuse and localized).
Primary tumors of the optic nerve are usually observed in patients of childhood and adolescence and are rare. Among primary tumors of the optic nerve, gliomas rank first in frequency and account for 80%, meningiomas 17% and neurofibromas 3%.
Meningioma
The initial concept of meningioma was introduced by Th. Leber in 1877. Over the past 100 years, the name of this tumor has changed. Cushing, believing that the tumor develops from the dura mater of the brain, in 1922 proposed calling it meningothelioma or arachnoid mesothelioma, and in 1962 L.I. Smirnov came to the conclusion that the source of growth of this tumor is arachnoid villi located between dura and arachnoid membranes. This allowed him to propose the term "arachnoidendothelioma". However, in the 70s of the XX century. The term “meningioma” was re-established.
Among all meningiomas of the central nervous system, optic nerve meningioma accounts for 1-2%. The tumor develops at the age of 20-60 years, more often in women; Meningiomas have been described in children that occur with more aggressive growth. Rapid tumor growth is also observed during pregnancy. As a rule, the tumor is unilateral, but cases of bilateral development of optic nerve meningioma have been described.
Clinic. Meningioma can grow along the entire length of the optic nerve trunk or have eccentric growth with invasion of the nerve sheaths. The direction of growth of meningioma in the orbit determines the clinical symptoms and the sequence of their development.
In the overwhelming majority of patients with meningioma, which has an infiltrative growth pattern, in the early stage the most typical pain is in the affected orbit and the same half of the head. The tumor grows into the dura mater of the brain and infiltrates the surrounding tissues, which is accompanied by limitation of the functions of the extraocular muscles. When the tumor reaches a significant size, swelling of the eyelids appears, exophthalmos is combined with red chemosis of the bulbar conjunctiva. It can be axial or offset, its size ranges from 6 to 14 mm. In the fundus there is a pronounced congestive optic disc.
With particularly rapid growth of the tumor on the disc and around it, there may be hemorrhages in the form of smears; in 1/3 of cases in such patients, optociliary shunts are formed, which are retinochoroidal collaterals on the optic nerve disc, which has been in a state of stagnation for a long time. The appearance of sharply dilated, bluish-colored veins on the stagnant disc indicates the spread of the tumor directly to the posterior pole of the eye. Visual impairment may be intermittent at first, and then progressively decreases. However, visual acuity can remain at a fairly high level for some time. Observations of patients with a similar pattern of tumor growth have shown that although their visual acuity is preserved, there is no hope for local tumor removal, since, by growing into the nerve sheath, meningioma forms tumor nodes in the extraocular muscles and orbital tissue.
With eccentric tumor growth, the visual field initially remains intact or asymmetrical areas of prolapse are observed according to the area of the tumor node. When meningioma grows concentrically to the optic nerve trunk and penetrates its tissue, a uniform narrowing of the visual field develops, and central vision deteriorates early (2-4 years before the onset of exophthalmos). Exophthalmos appears after a few months and even after 2-3 years; it is always axial, its size does not exceed 6-7 mm. The functions of the extraocular muscles are fully preserved. In the fundus, as a rule, primary optic nerve atrophy develops. An increase in the diameter of the optic nerve is accompanied by an increase in the size of its bone canal.
It is difficult to diagnose meningioma in such patients, since even on computer tomograms the optic nerve is not always enlarged enough to suggest tumor damage. Particularly difficult to diagnose is optic canal meningioma that grows into the orbit, which occurs in 5% of patients with optic nerve meningioma.
Morphogenesis. The tumor develops from arachnoid villi located between the dura mater and the arachnoid membrane. The optic nerve affected by the tumor increases in diameter by 4-6 times and can reach up to 50 mm in diameter. Macroscopically, the tumor has a grayish-pink color, the optic nerve trunk is usually well differentiated. When a tumor grows from the intervaginal space through the hard shell, successive infiltration of the orbital tissues appears and it is not possible to differentiate the optic nerve along its entire length in such cases.
Differential diagnosis. Optic nerve meningioma must be differentiated from any other perineurally located tumor if it grows eccentrically. With significant infiltration of retrobulbar tissues - from any pathological process that has a diffuse distribution, and primarily from a malignant tumor; with axial spread - from optic nerve gliomas.
Glioma
Glioma is an intradural formation, the tumor is represented by three types of cells: astrocytes, oligodendrocytes and macroglia. Based on their cellular structure, gliomas are divided into astrocytoma, which is called juvenile, since it develops in children, and oligodendroglioma, which more often affects adults. The first makes up 2/3 of all gliomas of the orbital segment of the optic nerve.
Davis identifies 5 stages of glioma growth
- Generalized hyperplasia of astrocytes and oligodendrocytes in the trunk of the optic nerve without disturbing its general structure, the membranes are intact.
- Increased proliferation of glia, membranes are involved in the process, but their integrity is not impaired, hyperplasia of arachnoid cells.
- Penetration of tumor cells into the intervaginal space of the gland with the formation of a mass of glial and arachnoid cells in it.
- Destruction of individual sections of the tumor membranes due to replacement with tumor tissue.
- The structure of the nerve is completely lost, the septa, sheaths and fibers of the nerve are completely destroyed.
A.F. Brovkina believes that, unlike meningioma, glioma never grows into the dura mater, however, along the trunk of the optic nerve, it can spread into the cranial cavity, reaching the chiasma.
Glioma is characterized by the formation in the orbit of a tumor node of various shapes: round, spindle-shaped, pear-shaped, sausage-shaped, with pronounced eccentric growth relative to the longitudinal axis of the nerve, it can be in the form of “beads” or “hourglass”. The size of the tumor in the orbit varies - from 1.5 by 2 cm to 4.5 by 5 cm. The tumor node is covered with a thick, smooth capsule and has a whitish or purple-bluish color. The tumor is dense on palpation, sometimes with partial cystic degeneration.
Glioma sometimes leaves a section of macroscopically normal nerve near the eyeball - a “neck”; more often the tumor has a wide base, equal to 2-4 diameters of the optic nerve, and comes close to the posterior pole of the eyeball.
Histological examination of removed tumors shows that they differ in their growth pattern in relation to the optic nerve and its membranes; intraneural growth is more often noted, and extraintraneural is less common.
- With the intraneural growth pattern, the nerve is diffusely infiltrated by tumor cells, the membranes are pushed to the periphery, the tumor does not grow into the hard shell “tumor in the capsule.” The soft membranes are loosened due to the proliferation of connective tissue and are germinated by tumor cells. Visual functions are preserved for a long time, since not all visual fibers are affected; some of them are pushed to the periphery by tumor cells and continue to function.
- With the extraneural growth pattern, the tumor consists of two parts - the extraneural part of the tumor is located between the soft and hard membranes and is fused to them, in the intraneural part of the tumor: the optic fibers are replaced by tumor tissue. Pressure from the extraneural part of the tumor leads to faster death of fibers. visual functions decrease quickly, ascending and descending atrophy of the optic nerve develops.
The clinical picture of glioma depends on the predominant localization of the tumor, which often coincides with its initial growth. There are two clinical groups: ON gliomas with intracranial spread and chiasmal gliomas. The primary localization of the tumor in the orbital part of the tumor is the most common. The first clinical sign of a tumor is a rapid decrease in vision almost to blindness; in young children, strabismus occurs, and there may be nystagmus.
Exophthalmos appears later, it can be axial and with displacement of the eyeball. Usually the eyeball protrudes forward and the mobility of the eye is not affected; later, as the tumor grows, the eye moves to the side and its mobility is limited. Impaired mobility of the eyeball is caused by the effect of the tumor on the extraocular muscles (pressure, stretching). The closer to the apex of the orbit the tumor is located, the earlier and to a greater extent the mobility of the eyeball is impaired. Repositioning the eyeball is difficult; with a high degree of exophthalmos, it is possible to palpate the tumor behind the eye.
There may be ophthalmological signs of difficulty in venous outflow from the orbit - swelling of the eyelids, dilation and injection of the episcleral vessels, decreased transparency of the maxillary sinus and ethmoid bone. If the tumor is large, its pressure on the sensitive endings of the trigeminal nerve in the orbit and ciliary nerves can cause sharp pain in the eyeball, decreased sensitivity of the cornea, and trophic changes in it. When the eyeball is compressed by a tumor in the anterior-posterior direction, hypermetropic refraction develops. Cases of increased IOP have been described.
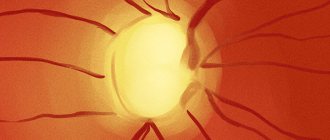
Changes in the fundus of the eye do not represent anything characteristic; they depend on the size, location, and duration of existence of the tumor. In the fundus, both congestive disc and optic nerve atrophy are equally often detected. At first, the phenomena of stagnation usually prevail, then its atrophy gradually develops.
With stagnation in the optic disc, tortuosity of the retinal vessels appears, and as a result of circulatory failure, optociliary shunts develop. As the tumor grows in the eyeball, swelling of the optic disc is especially pronounced, the veins are dilated, tortuous, and hemorrhages near the disc due to the developing obstruction of the central retinal vein. A pathognomonic sign of ON glioma is considered to be expansion of the ring of its bone canal, however, the absence of its expansion is not a sign of the tumor being limited to the orbital portion of the ON. A wide ring may also be due to the mechanical pressure of a large tumor reaching the apex of the orbit.
It is difficult to recognize the growth of glioma into the MN disc, because Most often, a congestive disc of the tumor develops on the side of the tumor. O. N. Sokolova believes that the spread of the tumor to the disc is manifested by the unevenness of the disc in different parts of it. Ophthalmoscopic symptoms of tumor spread to the optic disc are a delay in the contraction of the congestive disc of the optic nerve, the appearance of fresh hemorrhages on the disc and the periphery of the retina; as the swelling of the disc decreases, whitish, dense prominent masses and newly formed vessels become visible on it.
Signs of intracranial spread of ON gliomas are expansion of the ON canal, ophthalmological disorders in the other eye, indicating damage to the chiasm and the opposite ON, as well as the appearance of neurological symptoms. However, the detection of these symptoms indicates a large spread of the tumor; the initial stages of intracranial tumor spread are asymptomatic.
Diagnostic methods
The diagnosis of meningioma is established based on an analysis of the sequence of appearance of clinical symptoms and ultrasound scanning data, which makes it possible to determine the enlarged optic canal. The most informative is CT, in which the enlarged orbital segment of the optic nerve is always clearly differentiated and the border of its distribution is clearly visible. The tomographic picture is more complex with an infiltrative growth pattern, especially with an asymmetrical position of the tumor node. In such cases, an erroneous diagnosis of a perineural tumor is possible. It must be emphasized that CT for tumors of the optic nerve has significant advantages over MRI. In particularly difficult cases, TIAB provides assistance in establishing a diagnosis.
For many years, the pathognomonic sign of optic nerve glioma CT allows not only to visually observe the fusiform or cylindrical enlargement of the optic nerve in the orbit, but also to judge its spread along the optic canal into the cranial cavity. Ultrasound scanning is not informative enough, since it represents only the proximal and middle third of the optic nerve. MRI is more informative for intracranial tumor spread.
Standard list of studies for an accurate diagnosis
- Visometry,
- Perimetry
- Fundus ophthalmoscopy
- Ultrasound examination of the orbit
- X-ray of the orbit and brain with a focus on the visual canals according to Rese
- MRI of the brain and orbit
- CT scan of the brain and orbit
- Fine-needle aspiration biopsy, computed tomography-guided
- Contrasting veins of the eyeball
- Pneumocisternography of the chiasmal cisterns at the base of the brain
- Tumor examination during surgery
- Morphological study
Treatment
treatment of meningiomas within healthy tissue is effective in cases where the tumor is limited to the optic nerve sheaths, when computed tomograms show areas of unaffected optic nerve in the distal part.
Since the late 80s of the XX century. use radiation therapy to the area of the affected orbit with a total dose of at least 50 Gy. The progression of the process slows down, visual acuity remains unchanged for 5-6 years.
The prognosis for vision is unfavorable. When the tumor grows along the optic nerve trunk, there is a threat of its spreading into the cranial cavity and damage to the optic chiasm. The prognosis for life is favorable if the tumor is confined to the orbital cavity.
Given the extremely slow growth of optic nerve glioma, the choice of treatment method should be strictly individual. If vision is preserved and the patient can be monitored, an alternative to long-term observation can be radiation therapy, after which stabilization of tumor growth is noted, and in 75% of patients, vision even improves.
Radiation therapy is also indicated in cases where radical surgical treatment is impossible or the patient or his relatives refuse surgery. Surgical treatment is indicated when the tumor is limited to the orbital segment of the optic nerve in cases of sudden or rapidly progressive vision loss. The issue of saving the eye is decided before surgery. If the tumor grows to the scleral ring, which is clearly visible on computed tomograms, the affected optic nerve must be removed along with the eye, and the child’s parents must be warned about this.
If the tumor spreads into the optic canal or into the cranial cavity, the neurosurgeon decides on the possibility of surgical intervention. For malignant glioma, treatment is futile.
The prognosis for vision is always poor. The prognosis for life depends on the spread of the tumor into the cranial cavity. If the optic chiasm is involved, the mortality rate reaches 20%. When spreading to the hypothalamus and third ventricle, mortality increases to 55%. The prognosis becomes especially worse when a malignant variant of glioma, glioblastoma, occurs. Life expectancy from the moment the first symptoms appear does not exceed 6-9 months.
Diagnostics
Optic nerve glioma develops slowly and characteristic symptoms usually appear in advanced stages, when it is no longer possible to regain lost vision. Therefore, it is important to detect and fix the problem in a timely manner. You should consult a doctor for diagnosis as soon as a deterioration in the quality of vision becomes noticeable.
Based on the complaints, the specialist will be able to predict the development of the pathological process. However, in order to make an accurate diagnosis, this is not enough; a number of instrumental studies are necessary:
- ophthalmoscopy;
- visometry;
- perimetry;
- biomicroscopy;
- ultrasonography;
- radiography.
The most accurate methods for diagnosing benign formations of the optic nerve are CT and MRI. Tomography allows you to verify the presence of a tumor, as well as determine its exact location, structure and degree of activity of spread, germination into the skull area. A tissue biopsy and subsequent histological examination are also required.
Such diagnostic measures are necessary to determine the nature of the neoplasm.
Diagnosis of the disease
The disease can be defeated in the initial stages of formation, so it is worth observing the symptoms that appear and immediately contacting the clinic.
Diagnosis of the disease consists of prescribing a list of procedures:
- A neurologist, oncologist and therapist conduct an initial examination of the patient and collect a complete medical history.
- Electromyography with electroneurography can detect disorders in the area of the neuromuscular system.
- An echoencephalography procedure can detect hydrocephalus with changes in the midbrain structures.
- An ophthalmologist is able to recognize a tumor of the chiasm or optic nerve - a consultation with a specialist is prescribed.
- Electroencephalography is required in the presence of muscle cramps.
- Magnetic resonance therapy (MRI) reveals the location, shape and size of the tumor.
- Angiography examines the extent of damage to the blood vessels of the brain.
- Computed tomography is often used as an adjunct to MRI.
- Lumbar puncture with the collection of biological material allows you to study the structure of cells for malignancy.
- Blood and urine are examined in the laboratory for changes in essential elements.
The doctor will make an accurate diagnosis after receiving all the tests and a detailed study of laboratory test results. Treatment is selected for each patient individually.
Treatment options
It is impossible to get rid of optic nerve glioma using a conservative method. Treatment of the tumor can be carried out in the following ways.
Radiation therapy
One of the most effective methods of treating optic nerve glioma, which is carried out in the early stages. Indications for irradiation are small tumor sizes and intraorbital location. Not only the tumor, but also 2 cm around it is exposed to irradiation. In most cases, the prognosis is positive, the glioma stops growing, and vision is preserved.
However, it should be borne in mind that radiation therapy can cause various side effects, especially in childhood, when the body is still fragile.
Surgical intervention
The operation is performed if the patient’s vision is rapidly deteriorating or there is a high risk of complications. The complexity of surgery depends on the volume of the tumor:
- Small tumors are removed through orbitotomy. Sometimes resection of the damaged portion of the optic nerve is performed.
- Gliomas that have reached the scleral ring and continue to grow are eliminated by enucleation of the eyeball. To achieve a greater effect, enucleation is performed followed by the formation of a supporting stump.
In cases where the tumor grows into the cranial cavity, the decision about the possibility of surgery is made by a neurosurgeon.
Chemotherapy
It is performed after surgery to destroy any remaining cancer cells. The patient is prescribed a course of medications, in particular, glucocorticosteroids should be taken, which help reduce swelling of the skull. This is especially necessary if the cancer spreads to other parts of the brain.
However, due to the fact that such medications stop cell growth, this negatively affects the condition of the entire body. Therefore, doctors most often combine chemotherapy with radiation.
This method of treatment has many side effects, as a result of which it is not recommended in childhood.
Optic nerve glioma (meningioma): symptoms, causes, treatment, prevention
Optic nerve glioma is a pathology that often occurs, mostly in children. This disease is serious and can greatly affect your overall health. Treatment methods are most often drastic, but the prognosis can be positive if you consult a doctor early.
What is optic nerve glioma
Optic nerve glioma is a rare pathology that occurs in young and middle-aged children. This is a type of eye tumor.
Among all eye tumors they account for 35%; recently, statistics have recorded the appearance of glioma in adult patients over 20 years of age. But the average age is still 6-7 years.
With this disease, the tumor can be located in any part of the optic nerve and even go deep into the skull.
The disease usually originates in the glial components of the optic nerve. This is a small area, but the development of a tumor in this location can have serious consequences, especially for visual function.
Causes
Until now, doctors are 100% unaware of the causes of glioma. The tumor is thought to result from neurofibromatosis type I. Neurofibromatosis is an inherited disease that increases susceptibility to tumor development.
In this case, fusiform expansions of the optic nerve are visible on diagnostic images, and the tumor is localized on both sides. The course of the disease can be asymptomatic and is discovered by chance when checking visual acuity.
There may also be a hereditary predisposition. If your family has had problems with similar diseases, you should regularly consult an ophthalmologist and monitor the state of your visual function.
Treatment
There are several treatment options. Radiation is considered one of the most effective, since this type of tumor is very sensitive to radiation.
In addition, treatment is carried out with chemotherapy and surgery. Each method has its own characteristics:
- Radiation therapy is carried out in the early stages. The entire glioma plus 2 cm around it is irradiated. In most cases, the prognosis for vision is positive, but the method has many side effects, and children do not always tolerate radiation well. It all depends on the strength of the immune system and the child’s body.
- Chemotherapy. - with the help of medications, the growth of tumor cells is stopped, but in this case, the general state of health also worsens. The greatest effect is achieved in combination with radiation therapy.
- Surgery - surgical removal of the tumor. This radical method is prescribed for sudden and progressive deterioration of vision.
The work of surgeons can be carried out using several methods. For intraorbital glioma, an orbitotomy is performed and the entire portion of the affected nerve is removed. In severe cases, the eye will have to be removed.
If the tumor is intracranial, then trephination of the frontal part of the skull has to be performed. The intraorbital and intracranial part of the glioma is removed. Surgical intervention is carried out by neurosurgeons after they decide on the real need for such intervention.
Complications
It is important to treat the disease correctly. If you do not follow the specialist’s instructions, the following complications may occur:
- Atrophy of the affected nerve. Leads to a narrowing of the field of vision, impaired color perception, loss of complete or partial vision.
- Keratitis is inflammation of the cornea. Manifests itself in constant redness of the eyes due to vascular changes.
- Dry eyes.
- Loss of visual function.
In cases where the tumor grows to the ocular junction, death is quite possible.
Prevention
The main method of prevention is timely diagnosis and treatment of a benign tumor. Parents should not neglect scheduled visits to the ophthalmologist, who, if there is any suspicion of the presence of glioma, will prescribe additional tests.
Parents should understand that displacement of the eyeball and its bulging characterizes an already complicated stage. It is important to recognize the disease as soon as the tumor has affected the glia, preventing it from spreading deep into the skull or throughout the optic nerve. If a child often complains of pain in the eyes, consult a doctor immediately.
Optic nerve glioma is a complex disease that can result in blindness or even death of the patient. For a positive prognosis, it is important to contact a specialist in the early stages of the tumor and begin treatment immediately. Then it is possible to avoid surgery and removal of the eye, and also preserve vision, at least partially.
Since there are very few symptoms and they manifest themselves in an advanced form of the disease, parents are advised to adhere to scheduled visits to the ophthalmologist as much as possible and monitor the child’s vision. It is necessary not to ignore the child’s complaints of pain in the eyes and head.
Source: https://onkologia.ru/dobrokachestvennyie-opuholi/organy-zreniya/glioma-zritelnogo-nerva/
Forecast
Optic nerve glioma is a dangerous disease that, if not treated promptly, leads to complete loss of vision in one or both eyes. The prognosis for this disease depends on the extent of the cancer process and the size of the tumor. If the pathology was detected at the initial stage of development, then with proper therapy, vision can be at least partially preserved. If the problem is detected in the later stages, the prognosis is extremely unfavorable.
Author of the article: Kvasha Anastasia Pavlovna, specialist for the website glazalik.ru Share your experience and opinion in the comments.
Prices
| Disease | Approximate price, $ |
| Prices for diagnosing migraine | 7 060 — 8 260 |
| Prices for diagnosing childhood epilepsy | 3 100 — 4 900 |
| Prices for brain shunting for hydrocephalus | 33 180 |
| Prices for treatment of Parkinson's disease | 58 600 |
| Prices for migraine treatment | 9 680 |
| Prices for the diagnosis of amyotrophic lateral sclerosis | 6 550 |
| Prices for diagnosing epilepsy | 3 520 |
| Prices for rehabilitation after a stroke | 78 300 — 82 170 |
| Prices for treatment of childhood epilepsy | 3 750 — 5 450 |
| Prices for treatment of multiple sclerosis | 4 990 — 17 300 |
| Disease | Approximate price, $ |
| Prices for strabismus treatment | 14 190 |
| Prices for treatment of eye melanoma | 8 000 |
| Prices for treatment of keratoconus | 27 610 — 59 950 |
| Prices for cataract treatment | 8 690 |
| Prices for glaucoma treatment | 7 260 — 8 360 |
| Disease | Approximate price, $ |
| Prices for thyroid cancer screening | 3 850 — 5 740 |
| Prices for examination and treatment for testicular cancer | 3 730 — 39 940 |
| Prices for examinations for stomach cancer | 5 730 |
| Prices for diagnosing esophageal cancer | 14 380 — 18 120 |
| Prices for diagnosis and treatment of ovarian cancer | 5 270 — 5 570 |
| Prices for diagnosing gastrointestinal cancer | 4 700 — 6 200 |
| Prices for breast cancer diagnostics | 650 — 5 820 |
| Prices for diagnosis and treatment of myeloblastic leukemia | 9 600 — 173 000 |
| Prices for treatment of Vater's nipple cancer | 81 600 — 84 620 |
| Prices for treatment of colorectal cancer | 66 990 — 75 790 |
| Prices for treatment of pancreatic cancer | 53 890 — 72 590 |
| Prices for treatment of esophageal cancer | 61 010 — 81 010 |
| Prices for liver cancer treatment | 55 960 — 114 060 |
| Prices for treatment of gallbladder cancer | 7 920 — 26 820 |
| Prices for treatment of stomach cancer | 58 820 |
| Prices for diagnosis and treatment of myelodysplastic syndrome | 9 250 — 29 450 |
| Prices for leukemia treatment | 271 400 — 324 000 |
| Prices for thymoma treatment | 34 530 |
| Prices for lung cancer treatment | 35 600 — 39 700 |
| Prices for melanoma treatment | 32 620 — 57 620 |
| Prices for treatment of basal cell carcinoma | 7 700 — 8 800 |
| Prices for the treatment of malignant skin tumors | 4 420 — 5 420 |
| Prices for treatment of eye melanoma | 8 000 |
| Prices for craniotomy | 43 490 — 44 090 |
| Prices for thyroid cancer treatment | 64 020 — 72 770 |
| Prices for treatment of bone and soft tissue cancer | 61 340 — 72 590 |
| Prices for treatment of laryngeal cancer | 6 170 — 77 000 |
| Testicular cancer treatment prices | 15 410 |
| Bladder cancer treatment prices | 21 280 — 59 930 |
| Prices for cervical cancer treatment | 12 650 — 26 610 |
| Prices for treatment of uterine cancer | 27 550 — 29 110 |
| Prices for treatment of ovarian cancer | 32 140 — 34 340 |
| Prices for treatment of colon cancer | 45 330 |
| Prices for lymphoma treatment | 11 650 — 135 860 |
| Prices for kidney cancer treatment | 28 720 — 32 720 |
| Prices for breast reconstruction after cancer treatment | 41 130 — 59 740 |
| Prices for breast cancer treatment | 26 860 — 28 900 |
| Prices for prostate cancer treatment | 23 490 — 66 010 |