Normally, the lens of the human eye is surrounded on all sides by the ligaments of Zinn, which maintain its stable position. The posterior and anterior gas chambers contain aqueous humor. The vitreous body is adjacent to the lens at the back.
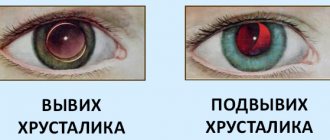
If the lens is displaced, it dislocates in space. This condition is called luxation or dislocation in ophthalmology. This pathology is accompanied by a violation of the volume of intraocular fluid, as well as displacement of the iris and pupil.
Lens dislocation during luxation can be partial or complete. Both cases are quite serious ophthalmological problems that need to be treated in a timely manner.
General information
The lens is an outwardly colorless convex lens in both directions. It is held in a constant position by a ligamentous layer, consisting of a large number of connective fibers associated with the ciliary muscle. If, due to a rupture or absence of this layer, the lens moves freely, this is called luxation. Cases of partial damage to the connecting fibers are called subluxation. During luxation, the lens moves uncontrollably and may end up in the anterior chamber of the eyeball. If the lens is found on the back side of the iris, it is called a vitreous lens shift.
Causes of pathology
The most common factor is injury. Doctors also identify the following reasons:
- congenital underdevelopment of the ophthalmic apple;
- genetic predisposition;
- degenerative processes;
- long-term inflammatory processes.
Return to contents
Types of disease
There are the following 2 types of eye lens luxation:
- This type of disease most often manifests itself in incomplete separation from the ciliary muscle. The lens is displaced into the vitreous body, and incomplete dislocation occurs with one side leaving its normal state. In the case of partial dislocation, a significant decrease in vision is observed and retinal detachment occurs. Cases of complete displacement are extremely rare and occur due to serious injuries or underdevelopment of the eyeball in the fetus.
- Luxation of the lens into the anterior or posterior zone of the eyeball chamber is accompanied by an almost complete loss of the usual location of the lens. There is a strong impact on the iris, the hydrostatics of the eye is disrupted, and because of this, the pressure inside the eye increases. With such a dislocation, the lens occupies the entire posterior or anterior chamber of the eyeball, causing loss of visual functions and deformation of the pupil.
Luxation is often a factor in the development of glaucoma.
↑ Marfan syndrome
Marfan syndrome is the most common cause of ectopic lens in children.
The type of inheritance is autosomal dominant. A mutation was discovered in the fibrillin gene 15q of chromosome 21.1. Clinical characteristics include:
- Cardiac changes - aortic aneurysm, dilatation of the aortic root, valve prolapse.
- Skeletal changes - tall stature, arachidactyly. scoliosis, chest deformation (Fig. 14.5).
- Ocular manifestations - ectopic lenses (usually upward dislocation), cataracts, high myopia, retinal detachment.
High myopia, observed in Marfan syndrome, is not only refractive, but also axial. Axial myopia is dangerous with a high risk of retinal detachment, not only during cataract surgery, but also in everyday life (Fig. 14.6).
Effective treatment method
If the doctor determines that the lens has partially shifted into the vitreous body, the wearing of specialized lenses will be indicated. After a certain period of time, the ophthalmologist will be able to determine the effectiveness of such therapy. If it has a positive result, the conservative treatment method continues with the prescription of eye drops or other medications, which are determined purely individually for each patient. In cases of complications or unsatisfactory results, surgery will be indicated. Such operations are performed in a hospital; if there are contraindications to surgical intervention, the method of laser coagulation is proposed.
If the lens is completely torn off, surgery is necessary.
If a complicated form of pathology or complete separation of the lens from the ciliary muscle is observed, a surgical treatment method is immediately prescribed after undergoing additional specialists. In such situations, the lens is removed and replaced with an artificial one; it is attached to the muscle with special synthetic fibers. In this case, the function of the eye can be completely preserved. But such operations can be complicated by the following side effects:
- expulsive hemorrhage;
- retinal destruction;
- mydriasis;
- hyephema, etc.
Return to contents
↑ Persistent primary vitreous hyperplasia (PVH)
This term is used to describe a wide range of congenital anomalies, including:
- microphthalmos;
- shallow anterior chamber;
- elongated ciliary processes;
- cataract;
- retinal detachment;
- retrolental membrane;
- intralenticular hemorrhages.
Typically, PHPS occurs as a unilateral lesion. Cataracts that do not reduce visual acuity at birth tend to progress later. In some cases, surgical treatment gives a good visual effect, but there is a risk of postoperative complications. The disease is often complicated by glaucoma (Fig. 14.3).
Lens dislocation
The term “lens luxation” is used to describe its complete dislocation. Subluxation is a partial displacement of the lens. In children, subluxation of the lens is fraught with a decrease in visual acuity and the occurrence of amblyopia. Luxation of the lens forward can provoke pupillary block and, as a result, glaucoma and corneal edema. There are the following causes of lens dislocation.
Homocystinuria
Pathology of metnonine metabolism related to deficiency of cystatinoinin B synstase. Patients have elevated levels of homocystine and methionine in the blood and urine. The diagnosis is made based on the identification of homocystine in the urine using bicarbonate and itroprusside.
Homocystinuria is characterized (Fig. 14.4):
- arachnodactyly;
- rushes of blood to the cheeks;
- blond hair;
- mental retardation; • tendency to thromboembolism:
- ectopia of the lens (usually downward and/or forward).
Early diagnosis and timely initiation of treatment are extremely important, since there are no clinical manifestations of this disease at birth.
Therapy includes:
- high doses of pyridoxine;
- betaine;
- metpopin in small doses;
- a diet high in cysteine;
A high level of hydration is required during surgery.
Possible complications
In cases of timely access to a medical institution and the selection of adequate therapy, the chances of complete preservation of vision are quite high. But in especially severe cases, it is almost impossible to restore visual functions. This is due to the fact that after injury there is a strong surge in pressure inside the eye, which destabilizes the internal structure of the eyeball. This pathology leads to damage to the iris, visual nerve, vascular layer and retinal detachment. Against the background of stress, they quickly progress and become irreversible.
Lens luxation
Normally, the lens is surrounded on all sides by the ligaments of Zinn, which maintain it in a stable state. The posterior and anterior chambers of the eyeball are filled with aqueous humor. The vitreous body is located behind the lens.
When the lens is displaced, it becomes dislocated in space, which is called luxation, or dislocation. This pathological condition is accompanied by an imbalance of intraocular fluid, displacement of the pupil and iris.
Luxation of the lens may be associated with congenital pathologies in which the zonules of Zinn are underdeveloped or partially absent. Also, lens dislocation can be caused by ligament rupture due to injury, degenerative process, etc.
There are two types of lens luxation:
1. In the first type, the lens dislocates towards the vitreous. In this case, with subluxation, the lens is displaced into the pupillary area, occupying less or more than half of its diameter. During the examination, you can visualize the displaced lens itself, namely, its convex edge. The direction of luxation can be symmetrical or asymmetrical. The substance of the lens in some cases remains transparent, and sometimes becomes slightly cloudy.
Complete dislocation of the lens with this type of displacement is not common. This usually occurs with any congenital anomalies in the structure of the eyeball. With partial dislocation, a significant decrease in vision occurs, retinal detachment occurs, and trembling of the iris occurs. Also, against the background of displacement of the lens into the vitreous region, other serious pathologies of the eye can develop.
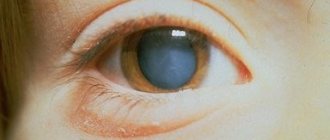
2. Displacement of the lens into the space of the anterior or posterior chamber is accompanied by almost complete dislocation of the lens. At the same time, the lens itself puts quite a lot of pressure on the iris. This condition can lead to the development of an acute inflammatory reaction, damage to the cornea, pupil constriction often occurs, as well as glaucoma (primary or secondary). Being in the anterior or posterior chamber, the lens creates an obstacle to the normal circulation of aqueous humor. As a result, intraocular pressure increases. The lens can be visualized deep in the eye chambers as a cloudy spherical drop. With complete dislocation, the lens occupies the entire posterior or entire anterior chamber of the eye, which leads to deformation of the pupil and a significant decrease in visual acuity.
Etiology of ectopic lens
Ectopia of the lens (lat. Ectopia lentis) is a complete or partial displacement of the lens from its usual position, caused by a separation of the zonules. In this case, the lens can shift (luxurize) both into the anterior and posterior chambers (Fig. 1).
The etiological factors causing lens ectopia are completely different in different animal species [1].
In humans, the main cause of lens luxation is direct traumatic contusion of the eyeball, which leads to its displacement into the vitreous body. In second place in the incidence of lens ectopia are genetic diseases: Marfan syndrome (spider finger syndrome) (Fig. 2) and Weill-Marchesani syndrome (Weill-Marchesani), characterized by growth retardation, brachydactyly with sedentary joints and mental retardation. Age-related dysfunctions of the ligaments of Zinn occupy the last place in the occurrence of ectopia in humans [9].
In dogs, the main causes of lens luxation are hereditary diseases, primarily PLL, to which terriers and related breeds, miniature bull terriers, Chinese Crested dogs, Shar Peis, etc. are predisposed. The disease is transmitted in an autosomal recessive manner. This pathology manifests itself between the ages of 3 and 8 years (on average 4...5 years), bilaterally; After lens luxation occurs in one eye, in the other it usually develops after 1…3 months. According to our observations, with PLL, in approximately 60% of dogs the lens dislocates into the vitreous, and in 40% into the anterior chamber. The lens moves into the anterior chamber when the anterior layers of the vitreous body are dense, and they seem to push the torn lens forward. With syneresis (liquefaction of the vitreous body) or a violation of the integrity of the anterior hyaloid membrane, the dislocated lens, on the contrary, moves back, deep into the vitreous body. In some cases, the lens may luxate onto the fundus [1, 4, 5].
Rice. 1. Ectopia (complete dislocation) of the lens into the anterior chamber in a cat
Rice. 2. Dislocation of the lens into the vitreous body in humans with Marfan syndrome
Rice. 3. Dislocation of the lens into the anterior chamber in an 8-year-old Yorkshire terrier with overripe cataracts. Atrophy of the eyeball develops against the background of lens-induced uveitis and hypotension
Rice. 4. Dislocation of the lens into the anterior chamber in an 11-year-old cat due to chronic uveitis. The iris is edematous, the vessels are dilated, deep corneal vascularization is visualized in the lower segment
Rice. 5. Complications of lens luxation into the anterior chamber in a 4-year-old dog with PLL. A corneal cataract forms in the lower segment and phacotopic glaucoma (IOP 36 mm)
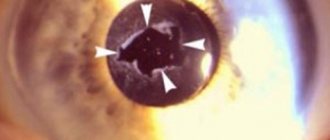
Rice. 6. Subluxation of the lens of the 1st degree. The initial aphakic crescent is identified (marked with an arrow), the anterior chamber is locally deepened at the site of ligament rupture
Overmature cataracts in dogs also often lead to ectopic lens (Fig. 3); accompanied by signs of sclerosis and calcification of the lens [1]. The calcified lens begins to decrease in volume, the load on its zonular ligaments increases, which begin to tear off. The formation of lens subluxation when cataracts mature is not uncommon, so it is safer and more expedient to operate cataracts in dogs at earlier stages [2].
In cats, the etiology of lens ectopia differs from that in humans and dogs (Fig. 4). In them, the main reason for luxation into the anterior chamber is chronic uveitis (develops at the age of 9...11 years), and into the posterior chamber - glaucoma. Hereditary luxations occur only in 2.5% of cases [3].
Diagnosis and treatment
Before a doctor prescribes treatment for a patient with lens luxation, he must conduct a full examination of his visual function, including determination of acuity and visual fields. The ophthalmologist also performs a visual examination of the eyeball as a whole, the cornea, pupil, adnexal and central apparatus, and assesses the condition of the palpebral fissures and eyelids. The complex of mandatory methods includes determining the reaction to light, which is associated with the peculiarity of the function of the lens, which is one of the main light-conducting organs in the eyeball.
If the doctor determines a slight displacement of the lens, then you can get by with the use of special lenses. While wearing corrective lenses, the doctor assesses the degree of restoration of visual function. If the effectiveness of such treatment is low or if any complications develop, they move on to the next stage of treatment, which includes a surgical technique. Surgery to restore a dislocated lens is usually performed in an inpatient setting. If it is impossible to perform extensive surgery, the patient is prescribed laser coagulation, which improves visual function for a fairly long period of time.
In case of complicated lens dislocation, the patient is prescribed a number of additional tests and examinations. Next, surgical treatment is performed. For example, in secondary glaucoma, the surgeon removes your own lens and replaces it with an artificial lens.
After such operations, side effects often occur, which include damage to the endothelial lining of the cornea, destruction of the retina, expulsive hemorrhage, ocular hyphema, pupillary mydriasis, loss of the vitreous body, etc.
Possible complications
The treatment plan for lens luxation is drawn up on an individual basis and largely depends on the neglect and severity of the condition. With timely detection of the disease and rational therapy, the prognosis for patients is much better. In this case, it is often possible to achieve a lasting positive reaction. If the patient does not react in time to decreased vision, and the doctor does not prescribe treatment for lens dislocation, the pathological process can lead to complete blindness. Particularly serious consequences occur when the lens is completely dislocated into the anterior or posterior chambers of the eye. This is due to a violation of the passage of intraocular fluid, which often leads to inversion of the iris, pathological damage to the optic nerve, retinal detachment, damage to the cornea or choroid. All these conditions progress rapidly and are irreversible.
After serious traumatic consequences, severe consequences are also quite stable. In this case, lens dislocation is often accompanied by blindness and the formation of psychological problems. If the patient seeks ophthalmological help in time, the chances of restoring visual function increase.
Subluxation (subluxation) and dislocation (luxation) of the lens into the vitreous body - causes and treatment
Lens luxation is the complete separation of the lens from the suspensory ligament. In this case, the lens moves into the anterior or posterior chamber of the eye. At the same time, visual acuity decreases because the structure of the optical system is disrupted, from which a lens with a power of 19 diopters falls out. If the lens is dislocated, it must be removed.
When the lens is subluxated, there is only a partial separation of the ligament of Zinn, the extent of which can vary.
Dislocations and subluxations can be congenital or acquired pathological conditions. The last type of lens displacement is associated with blunt trauma to the eye, severe concussion. Clinical manifestations directly depend on the severity of the resulting defect. In particular, minimal damage often goes unnoticed. This is possible if there is no damage to the anterior limiting membrane of the vitreous body and the lens remains transparent.
The main symptom of lens subluxation is iris trembling, also called iridodonesis. The iris tissue is quite delicate and normally rests on the anterior pole of the lens. If there is a slight displacement of the lens, then its vibration is transmitted to the iris. Sometimes this symptom is noticeable even without the use of special research methods. In other cases, observation of the iris in lateral illumination or using a slit lamp is required. This helps to detect even slight displacement of the iris. If you move your eye sharply to the left or right, the vibrations of the iris cannot be detected. Interestingly, iridodonesis is not always present, even if there is noticeable displacement of the lens. This is due to the fact that along with a tear of the ligament of Zinn, a defect in the anterior limiting membrane of the vitreous body occurs. This leads to the appearance of a strangulated vitreous hernia, plugging the resulting hole. This leads to a decrease in the mobility of the lens.
If there is no iris trembling, then subluxation is determined by other symptoms that become noticeable during biomicroscopy. Such signs include uneven depth of the anterior and posterior chambers of the eyeball, which is associated with pressure and anterior displacement of the vitreous substance in the area of weakening of the lens support. If there is a strangulated hernia fixed by adhesions, then the size of the posterior chamber increases, and the anterior chamber, accordingly, decreases in this area.
During examination, the posterior chamber remains inaccessible to inspection, therefore, to assess its depth, an indirect sign is used (the distance from the edge of the pupil to the lens on all sides).
If the subluxation of the lens is uncomplicated, then a significant decrease in visual acuity is not observed. In this case, no treatment is required. Sometimes a subluxated lens reduces its transparency. It can also cause the development of secondary intraocular hypertension leading to glaucoma. In this case, it is optimal to remove the modified lens. In order to correctly determine the tactics of surgical treatment, if possible, strengthen the lens capsule for subsequent placement of an artificial lens in it. It is necessary to carry out early diagnosis of the disease.
Content:
- 1 Persistent primary vitreous hyperplasia (PVH)
- 2 Marfan syndrome
- 3 Weil-Marquesani syndrome
- 4 Cataract
Description
Anatomy and embryology
The lens is a biconvex optical element of the refractive system of the eye, located behind the iris and in front of the vitreous body. The stable position of the lens is ensured by the ligamentous apparatus coming from the ciliary body. At birth, the equatorial diameter of the lens is 6.5 mm, and the anteroposterior diameter is 3.5 mm. In adulthood, the equatorial diameter of the lens increases to 9 mm, and the anteroposterior size - to 5 mm. The posterior surface of the lens bag is covered with columnar epithelial cells that produce primary lens fibers. The lens capsule is formed by the basement membrane of the lens epithelium.
Developmental anomalies
A long list of developmental defects includes the following anomalies in the size, shape, position and transparency of the lens
- Congenital aphakia. It occurs as a primary disorder of the development of the lens and as a secondary spontaneous absorption. In both cases, visual acuity is usually low due to concomitant malformations of other structures of the eyeball.
- Double lens is a rare pathology caused by corneal metaplasia and coloboma.
- Colobomas of the lens - occur as an isolated defect (usually unilateral) and in combination with colobomas of other structures (usually bilateral pathology) (Fig. 14.1).
- Microspherophakia (Fig. 14.2) is an anomaly in which the lens is reduced in diameter and has a spherical shape. It occurs as an isolated defect or is part of the symptom complex of Weil-Marchesani syndrome.
- Lenticonus is an axial deformation of the posterior surface of the lens and is often associated with progressive cataracts. Being, as a rule, a unilateral pathology, it is inherited in an autosomal recessive manner or an X-linked recessive trait.
- Anterior lenticonus is an axial deformation of the anterior lens capsule, usually without accompanying cataracts affecting visual acuity. Included in the symptom complex of Alport syndrome, together with hereditary nephritis and sensory hearing loss. The disease is determined by a gene localized on the X chromosome. A mutation was discovered in the collagen gene COL4A5 at Xq22.
- Rudiment of the choroid of the lens. It looks like a spot on the posterior surface of the lens or an extensive network of rudimentary vessels attached to the posterior capsule (especially typical for premature babies).
Recommended clinics for cataract treatment
“Dr. Shilova’s Eye Clinic” is one of the leading ophthalmological centers in Moscow, where all modern methods of surgical treatment of cataracts are available. The latest equipment and recognized specialists are a guarantee of high results. Go to the organization's page in the catalog >>>
“MNTK named after Svyatoslav Fedorov” is a large ophthalmological complex “Eye Mycosurgery” with 10 branches in various cities of the Russian Federation, founded by Svyatoslav Nikolaevich Fedorov. Over the years of its work, more than 5 million people have received assistance. Go to the organization's page in the catalog >>>
“Helmholtz Institute of Eye Diseases” is the oldest research and medical state institution for ophthalmology. It employs more than 600 people who provide care to people with a wide range of diseases. Go to the organization's page in the catalog >>>
Luxation and subluxation of the lens (luxation and subluxation)
Luxation (subluxation) of the lens is not only a serious pathology in itself, but also carries the risk of developing dangerous complications. The lens capsule is supported by cyanoid ligaments. They provide the necessary geometric arrangement of this visual structure, and also participate in the process of accommodation. Partial (subluxation) or complete (luxation) dislocation of the lens occurs, respectively, with complete or partial rupture of the ligaments. As a result, the lens shifts towards the vitreous body or chambers of the eye. This leads to decreased vision and requires qualified assistance due to the risk of developing associated disorders.
Tactics of ophthalmological examination of animals with ectopic lens
If lens subluxation is suspected, a complete ophthalmological examination is necessary, which includes biomicroscopy of the anterior chamber on a narrow and wide pupil, tonometry, ophthalmoscopy, ultrasound (UBM), ERG.
They begin with biomicroscopy of the anterior chamber on a narrow pupil in transmitted light. The depth, uniformity of the anterior chamber, and the presence of vitreous humor in it are examined. For better visualization, the pupil is dilated (with normal IOP) and, under conditions of maximum mydriasis, under 16x magnification in focal lighting, the periphery of the lens and the condition of the ligaments are examined, directing the light from the side opposite to luxation. Then the fundus is examined to rule out retinal detachment and optic nerve atrophy. An indirect reverse ophthalmoscope of the Scapens type with lenses of 20 and 16 D is used. In opaque media, ultrasound of intraocular structures and ERG are mandatory.
Causes of luxation and subluxation of the lens
Insufficient development of cyanotic ligaments can be congenital. In this case, some of the fibers may be completely absent or there may be a functional insufficiency of the existing ligaments.
Acquired dislocation is often a consequence of injuries, degenerative and age-related changes, uneven decrease in the elasticity of the cyanotic ligaments, and inflammatory diseases affecting the lens capsule. The functional failure of the connecting apparatus can develop as a result of the systematic action of severe shocks and vibrations. A predisposition to lens malposition may be due to acquired cataracts and glaucoma.
Classification
Based on the direction of lens displacement, two types of luxation are distinguished:
1. Partial dislocation (subluxation) : the lens is displaced towards the vitreous body. With this type, only partial subluxation of the lens is most often observed. In this case, the displacement can be symmetrical or one-sided. The lens itself remains transparent or slightly clouded. Vision can be maintained at a sufficient level.
2. Complete dislocation : the lens is displaced into the anterior or posterior chamber. This disorder leads to compression of the iris, which can cause inflammation, damage to the cornea and the development of glaucoma. With this type, even incomplete luxation can lead to a significant loss of visual acuity.
According to the degree of pathology, a distinction is made between complete luxation (in the case of rupture of all ligaments around the circumference of the lens capsule) and subluxation of degrees I-III.
Depending on the severity of the subluxation, one or another symptom complex is observed.
↑ Weill-Marquesani syndrome
Weill-Marchesani syndrome is a rare disease inherited in an autosomal recessive manner, although an autosomal dominant form of inheritance also occurs.
Clinical characteristics include:
- short stature;
- brachycephaly:
- short fingers and toes;
- spherophakia (with lens dislocation usually forward);
- lens myopia.
Other symptoms associated with lens dislocation:
- aniridia;
- ectopia of the lens and pupil - an autosomal recessive syndrome in which the lens and pupil move in opposite directions;
- simple ectopia lens - inherited as an isolated autosomal dominant trait;
- sulfide oxidase deficiency - accompanied by lens dislocation, progressive muscle rigidity and early death;
- injury;
- glaucoma;
- xanthine oxidase deficiency – associated with low serum uric acid levels.
Treatment for lens dislocation
Treatment for lens dislocation must necessarily include visual rehabilitation and prevention of amblyopia. In cases where the lens is displaced forward, to avoid damage to the cornea and prevent the development of glaucoma, it may be necessary to surgically remove the dislocated lens.
With the advent of the closed eye lensvitrectomy technique, the rate of surgical complications has significantly decreased.
Treatment includes:
- Spectacle correction - indications for it are limited due to high refractive errors, which reduce the tolerance of spectacle correction in children.
- Contact correction is justified in the treatment of high degrees of myopia and aphakia.
- Pupil dilation - may be advisable both for optical purposes and for repositioning the lens displaced forward.
- Surgery - lensvitrectomy technique using a limbal approach or access through the pars plana of the ciliary body. The most common complication of surgical intervention is retinal detachment.
- The yttrium-aluminum-garnet (YAG) laser, a laser destruction of the lens ligaments, is used to displace the lens that partially covers the pupil area.
Symptoms and diagnosis of lens luxation
Minor subluxation may go unnoticed even by the patient himself. The key sign for subluxation of any degree is iris trembling (iridodonesis). Often this symptom is visible without the use of special diagnostic techniques. In less certain cases, they resort to observation in the beam of a slit lamp or with side illumination.
In certain cases, even special research methods do not reveal iridodenosis. Lens phacodonesis is not transmitted to the iris. Then biomicroscopy is used, which makes it possible to indirectly suggest luxation by the unevenness of the depth of the anterior or posterior chambers. Symptomatic diagnosis can reveal accommodation disorders, lens astigmatism, and secondary phacotopic glaucoma.
Treatment for luxation and subluxation of the lens
Lens luxation of one degree or another requires treatment to the extent that it affects the patient’s vision and carries the risk of complications. Preliminary diagnostics allows you to collect information about visual function, fields, changes in lens transparency, and photosensitivity. Minor subluxation can be corrected using special lenses. If there is no risk of developing glaucoma, visual acuity is sufficient and stable, no further treatment is required, and the patient only undergoes regular preventive examinations by an ophthalmologist.
Our ophthalmology center has all the capabilities to quickly and effectively solve the problem of lens dislocation using various methods. Experienced surgeons will quickly eliminate diseases and restore vision even in the most difficult cases!
In more complex cases, with high degrees of luxation and subluxation, surgical treatment is performed. The lens can be restored to its place if it is possible to surgically ensure its further stable position and functional viability.
If complications develop or there is no prospect of preserving the natural lens, they resort to its removal, strengthening of the capsule and installation of an intraocular lens.
As with any surgical treatment, in this case the risk of certain complications cannot be excluded, but luxation itself can be even more dangerous over time. Complicated by secondary glaucoma, the dislocation causes degenerative changes in the retina and threatens complete loss of vision. Other dangerous diseases that develop against the background of lens dislocation can be: inversion of the iris, impaired trophism of the optic nerve, retinal detachment, corneal damage and vascular insufficiency.
Timely diagnosis and proven treatment methods allow not only to do everything possible to eliminate the consequences of lens dislocation, but also to keep further dynamics under control, carry out surgical correction in a timely manner or take therapeutic measures to maintain a high quality of life for as long as possible.
Trifocal lenses. See the world in the smallest detail
Trifocal lenses can help solve these problems. They have not one, but three focuses: for near, for medium distance and for distance. The patient can get rid of glasses and contact lenses forever. A person sees perfectly in any situation, at any level of illumination. At work. On a rest.
The essence of the work of an ophthalmologist, including an ophthalmic surgeon, is to improve a person’s quality of life, help him enjoy all the colors of the world, and see the smallest details of surrounding objects.
Patients tell me that after implantation of trifocal lenses they felt a “second youth”. People note that they were not just given back, but, in the literal sense of the word, “created” excellent vision. Many patients with both myopia and farsightedness have been accustomed since childhood to poor vision and to frequent changes and purchases of glasses. Therefore, after implantation of trifocal lenses, a real “Wow” effect occurs. It’s hard for people to believe what quality of vision is and – most importantly! – quality of life is possible!