Myopia (myopia)
- a disease in which a person clearly sees objects located nearby, but objects located at some distance seem blurry and indistinct.
Methods for treating and correcting myopia in modern medicine are varied.
The choice of method depends on the degree of myopia, concomitant diseases and the wishes of the patient. Can't you see the license plate of the car and the leaves on the tree, or count the birds and stars in the sky?
Do you want to know whether it is possible to restore vision specifically in your case? We will conduct a full examination and answer all questions! Sign up for diagnostics at Realiz! >>>
- Causes of myopia
- Symptoms of myopia
- What types of myopia are there?
- Methods of correction and treatment
- Myopia in children
- Prevention
- Cost of laser treatment for myopia
- Reviews about the treatment of myopia at the Realize center
Is it necessary to treat low myopia?
Myopia in the initial stage is not considered a disease.
It can be corrected with glasses (not on a permanent basis) and contact lenses. The reason for this is the possibility of restoring visual acuity. This result is acceptable if it has decreased due to work schedule, diet, hormonal imbalance, or age-related characteristics.
With weak myopia, the vascular wall retains its integrity. A slight increase in the size of the eyeball and a shift in focus can be compensated for. Decreased vision requires attention. With myopia, the state of visual function is unstable.
Any unfavorable factor (illness, stress, injury, toxicosis) can cause progression of myopia. The most dangerous complication is retinal detachment and complete loss of vision.
But how the operation occurs for high myopia and how effective this procedure is is indicated here.
In the video, is it necessary to treat low myopia:
This is explained by the stretching of the eyeball in the longitudinal direction: the stronger the myopia, the larger the diameter. Ruptures of the choroid, hemorrhages, and atrophy of the optic nerve occur.
Prevention of myopia
Preventing the development and complications of myopia is possible if you adhere to certain rules, including the following important points:
- regular visits to the ophthalmologist to monitor the level of vision;
- use of vitamin complexes;
- performing eye exercises during the working period;
- examination using ultrasound to determine the longitudinal size of the eyeball;
- proper equipment and lighting of the workplace with natural light lamps;
- use of special glasses when working at a computer;
- avoiding heavy physical work, falls, sudden body movements;
- lead an active but moderate lifestyle, including outdoor activities;
- Eat properly and nutritiously, adding fruits and vegetables of bright red, purple, orange colors to your diet. And also greens rich in pigment (preference is given to spinach, celery, parsley, dill, etc.).
It is important to know! Various devices that work with color therapy and massage help prevent myopia. "Amblyocor" develops the natural ability of the brain to compensate for blurry images. With the help of “Rucheyok” - hardware prevention with a special lens - myopic processes are stabilized, the muscular system is trained, and accommodation develops.
Questions and answers
Question: Hello. I am 26 years old. Myopia from 18 years of age. Doesn't progress quickly. 02/2005 R −2.5 L −2.75 Examination took place during pregnancy before childbirth. 06/2007 underwent examination due to deterioration in sensations. R −3.00 L −3.25. Now I'm pregnant, but I haven't had my eyes examined yet (should I?). Tell me, please, what kind of myopia is contraindicated for me to give birth on my own and is it worth carrying out any additional examinations? Thank you. PS: I don’t wear glasses all the time, only when snowboarding or driving. Answer: The indication for excluding the 2nd stage of labor is complicated moderate myopia and high myopia. You need to consult an ophthalmologist to have your retina examined. If there are no gross changes in PVCRD (peripheral vitreochoreoretinal dystrophies), then you can give birth on your own. But they are different, the most dangerous: silent ruptures, retinoschisis, “lattice” dystrophy, “trace cochlea” dystrophy.
Question: Hello! I'm pregnant, 29 weeks. I have high myopia in both eyes (-11 left eye and −10.25 right eye). The diagnosis also reads: “Central chorioretinal dystrophy of the left eye.” I was interested in the question of possible physiological management of childbirth. I was examined at the Eye Therapy Center, I was allowed to give birth on my own, but the doctor at the district clinic assured me that I needed to have a cesarean section. Now I am tormented by doubts; I really would not like to go blind during childbirth. Is it possible to give birth yourself with such a diagnosis? Tell me, please! Answer: Your myopia is really high, but the determining factor (in terms of the eyes) is not so much the degree of myopia itself, but the presence and severity of vitreochorioretinal dystrophic manifestations. The final decision on the method of delivery is made by the attending obstetrician-gynecologist, taking into account all the circumstances, incl. and the conclusion of a retinologist (laser ophthalmic surgeon).
Question: Hello! I am 32 years old, currently pregnant, 15 weeks pregnant. There are problems with vision, and, naturally, I am concerned about the method of delivery - natural birth or cesarean section. I was diagnosed in two independent clinics, the diagnosis was the same: “Myopic astigmatism OD. Complex myopic astigmatism OS. Frost-like degeneration of the retina of both eyes.” The diagnosis is the same, but the recommendations differ - in one clinic they strongly recommended doing laser coagulation, in the second clinic they recommended not doing coagulation, only observation and said that there are no contraindications for natural childbirth. Is it still worth doing laser coagulation or not? And if you don’t, how big is the risk during natural childbirth? Answer: Frost-like retinal degeneration is not a risk form of PVRD and does not require laser coagulation. You have no contraindications for natural childbirth.
Question: The antenatal clinic referred me to an ophthalmologist for recommendations on the management of childbirth (age 30 years, 2nd pregnancy, 3rd trimester). The doctor wrote: “Childbirth with the exception of the period of pushing.” In fact, this is a referral for a cesarean section. During my last pregnancy (5 years ago), with a similar eye condition, another doctor wrote “natural birth,” which was done, and there was no damage to vision. Is such a harsh tactic really necessary for the eye condition described below? I would not want to do a cesarean section if there is no real need for it... Answer: High myopia is not a contraindication for independent delivery. Previous births also support the latter. You need to consult an ophthalmologist-retinologist (a specialist in retinal diseases), decide for yourself where to do this. If you live in Moscow, ask for a referral to the CDC corresponding to your place of registration or seek advice from an ophthalmology clinic.
To select the optimal means of vision correction during pregnancy, it is very important to contact a competent ophthalmologist-contactologist. You can view information about our ophthalmologists, as well as make an appointment and ask your questions here. You can view information about our ophthalmologists, as well as make an appointment and ask your questions here
You can view information about our ophthalmologists, as well as make an appointment and ask your questions here.
If you use contact lenses and would like to purchase them with home delivery at a time convenient for you, take advantage of the offer from Zakazlinz.ru - place an order now, enter 100310 when placing your order and receive a discount on your purchase.
Andrienko Gulnara Vladimirovna, ophthalmologist at the Zakazlinz.ru medical center
Cost of laser treatment for myopia
| Excimer laser vision correction during surgery on both eyes (cost for both eyes) | |
| LASIK or Lepto-LASIK for grade I myopia, astigmatism | 39,000 rub. |
| LASIK or Lepto-LASIK for grade II myopia, astigmatism | 41,000 rub. |
| LASIK or Lepto-LASIK for grade III myopia, astigmatism | 43,000 rub. |
| Excimer laser vision correction during surgery on one eye (cost per eye) | |
| LASIK or Lepto-LASIK for grade I myopia, astigmatism | RUB 21,500 |
| LASIK or Lepto-LASIK for grade II myopia, astigmatism | 22,500 rub. |
| LASIK or Lepto-LASIK for grade III myopia, astigmatism | RUB 23,500 |
| Excimer laser vision correction for myopia (taking into account astigmatism) using the PRK method | 18,000 rub. |
Sign up for diagnostics at Realiz! >>>
general information
Vision problems are widespread among both adults and children. Every year the number of patients increases. This is due to the large visual loads that a person receives when working at a computer, as well as using electronic devices at close range. The situation is aggravated by hereditary predisposition, bad habits, poor nutrition, and physical inactivity.
Myopia, or also called myopia, is a vision defect characterized by refractive error. A person sees objects located in the distance blurry, but near objects he sees clearly.
There are true and false myopia (spasm of accommodation). How to distinguish them from each other? False myopia is characterized by spastic contractions of the ciliary muscle. It is also called tired eye syndrome. Most often, the disease occurs in children and young people, which is explained by the specific structure of the accommodative apparatus.
The risk group includes people with systematic overstrain of the oculomotor muscles. This includes schoolchildren who have to read a lot, as well as young people who work at the computer for a long time. The formation of an accommodation spasm is impossible in older people, since age-related changes in the structure of the lens cause presbyopia, or farsightedness.
With false myopia, a person may think that his vision is deteriorating and he needs glasses. However, the spasm of accommodation is reversible, and vision will be restored after rest. Without medical education, it is very easy to distinguish between these two pathologies. If you mistakenly try to correct the spasm of accommodation with glasses, then after some time it will develop into true myopia.
Even a small degree of myopia brings significant discomfort. A person is unable to see the number of an approaching bus or recognize the face of a familiar person. The disease can develop into third degree myopia, which threatens vision loss and disability.
Progressive myopia often occurs in childhood and adolescence. However, it always begins with a mild visual impairment
That's why it's important to see an ophthalmologist when the first signs of myopia appear.
Prevention
Prevention is an important condition for preventing the development of myopia.
- Ensure a comfortable environment while working: sufficient lighting, the distance to the monitor or book is at least 30 cm.
- During prolonged visual stress, take periodic breaks and give your eyes a rest.
- Exercise your eyes regularly. The exercises are simple, you can repeat them 3-5 times almost anywhere: at work, at home, while walking. Gymnastics takes only 5-10 minutes, but it significantly helps relieve tension and strengthen the eye muscles.
- Visit an ophthalmologist for preventive purposes once every 2 years. And if you have symptoms (pain, discomfort, deterioration of color vision, narrowing of the field of vision), consult a doctor immediately.
Why do children's vision deteriorate?
Vision in children deteriorates due to two factors: congenital and acquired. The first include:
- Hereditary predisposition. A child is more likely to be nearsighted, farsighted, or astigmatic if one or both of their parents suffers from one of these eye conditions.
- Prematurity. According to medical statistics, in about a third of children born prematurely, their vision deteriorates over the years.
- Congenital pathologies and eye defects. Diseases such as cerebral palsy, hydrocephalus and many others can be accompanied by visual defects.
Among the acquired reasons:
- Large and constant loads on the visual apparatus. Children have to read constantly. They go to school and do homework. Prolonged strain caused by focusing on objects close to the eyes leads to increased intraocular pressure.
- Bad light. This reason is related to the previous one. It is necessary that the lighting in which the child studies is not too bright and not too dim. The pages of a notebook, book, or monitor should not create glare from the light falling on them.
- Spinal diseases and incorrect posture. With constant stooping, blood circulation in all organs, including the brain, worsens. As a result, the conductivity of the nerve fibers responsible for transmitting signals from the organs of vision to the brain is disrupted. To treat a child, you will need the help of an orthopedist and a neurologist.
- Low physical activity. Computers and smartphones are replacing games in the yard, sports and other activities related to physical activity, during which the organs are saturated with oxygen. Lack of oxygen is one of the main causes of decreased vision.
- Lack of vitamins. Among the vitamins and minerals that play a significant role in the functioning of vision: folic acid, iron, zinc, vitamins A, B, D. It is difficult to keep track of what a child eats outside the home. To reduce the harmful effects of junk food on his body, you need to create a healthy diet at home.
- Lack of prevention. All of the above factors can be leveled out through preventive measures, which many parents neglect due to lack of time and other reasons.
It is impossible to prevent all causes. If there is a possibility of their occurrence, children should be examined more often. Regular examinations with an ophthalmologist and compliance with all doctor’s instructions will help stop the development of visual pathology.
Spasms of accommodation and their significance for the development of myopia (Part 2)
Description
L.A. Dymshits (1963) imagines the emergence and development of myopia as follows.
- 1. Irreversible changes in the lens with an increase in their refractive power due to prolonged accommodation stress are an important factor for the development of weak and non-progressive forms of myopia in schoolchildren.
- 2. An increase in IOP from contraction of extraocular muscles is undoubted. Of particular importance are jerky lateral eye movements during reading when moving the gaze from the end of the read line to the beginning of a new one.
- 3. Congenital or acquired insufficient stability of the sclera plays a role.
- 4. Hereditary factors may also influence the development of myopia.
- 5. Unfavorable environmental factors are also of great importance.
Thus, L.A. Dymshits considers myopia as a disease that occurs under the influence of external factors in persons with a hereditary predisposition to it.
Accommodation-convergent-hydrodynamic theory of A.I. Dashevsky. The author distinguishes three types of myopia (according to genesis): hereditary, congenital and acquired. Hereditary myopia occurs in families. Congenital myopia is more often observed when there is no “family” history, but it is possible to find out that in the first 3-6 months of pregnancy the mother suffered some kind of disease and the born child has developmental anomalies, including congenital myopia.
Acquired myopia always begins with false myopia (spasm of accommodation), which then turns into axial myopia due to stretching of the posterior hemisphere and lengthening of the eye axis.
As a result of a multilateral study of the problem of myopia, the convergent-accommodative-hydrodynamic theory of pathogenesis by A. I. Dashevsky was created. The theory is based on the following signs: weakening of the ciliary muscle, turning into its spasm; occurs when the eyes are defocus and, as a consequence, inhibition of visual reflexes; unfavorable conditions for visual work at close range.
Etiological factors include factors characterizing the general condition of the body: previous diseases, chronic intoxications that contribute to the development of vegetative dystonia, refractive errors, hereditary factors. The second group of factors combines unfavorable conditions for visual work at close range: insufficient lighting, improper sitting position while reading and writing, irrational furniture at school and at home, improper daily routine and other hygienic factors. In the presence of factors of the first group, the ciliary muscle weakens, asthenopic phenomena develop and subsequent spasm of accommodation, as well as inhibition of visual reflexes - accommodative, convergent and pupillary. Factors of the second group cause optical discomfort. Taken together, they disrupt the binocular autofocus of the eyes.
A spasm of accommodation is necessarily accompanied by a spasm of the abductors and adductors of the eyes and an increase in IOP. It is interesting that E. Adamyuk wrote about this back in 1881.
Normally, during convergence, under the influence of the external rectus and both oblique muscles, the eyeball is deformed, somewhat lengthening along its axis. This deformation leads to an increase in IOP. Elongation of the axis leads to the appearance of temporary axial convergent myopia. For binocular fixation, a lower degree of lens myopia becomes necessary, which reduces the level of accommodative convergence, which is the “convergence response” to reduced lens accommodation. Accommodative convergence cannot provide complete rotation of both eyes to a fixed point. This convergence deficit, described in the literature as “physiological exophoria” without explanation of its causes, has received such an interpretation for the first time. The convergence deficiency is compensated by fusional convergence.
In order for the internal rectus muscle to contract for fusional convergence, the external rectus muscle must relax, as does the antagonist reciprocally associated with it. Normally this is what happens. When the adductors and abductors are in spasm, contraction of the former and especially relaxation of the latter is not easy. These changes in muscle tone lead to fluctuations in fusion and phoria, up to excesses of fusion, which causes increased optical discomfort and causes a desire to bring the text closer to the eyes, that is, to increase the angle of convergence.
Increased convergence means even greater deformation of the eyeball due to spasm of the external muscles and, therefore, contributes to an even greater increase in IOP. Areas of the sclera with an elongated radius, according to the laws of the study of resistance of materials, have less resistance. The jerky eye movements described by Cornberg (1951) during reading and writing further increase IOP, and after exceeding the limit of proportionality (according to Hooke's law), previously normally reversible microdeformations of the sclera become irreversible - residual. The appearance of residual microdeformations marks the beginning of the formation of axial myopia. In the future, the accommodative spasm accompanying axial myopia is the trigger for its progression. The changes described above cause new microdeformations of the sclera of the posterior hemisphere, which contributes to its further stretching.
Proof of this position of the theory of A.I. Dashevsky is the possibility of treating patients with axial myopia using methods of divergent disaccommodation and microfogging. We have a significant number of observations of patients in whom not only early, but also late pseudomyopia of 3.0-4.0 D was cured and visual acuity was brought to 1.0. It is also important that with axial myopia, even at 7.0-8.0 D, long-term and persistent treatment with these methods sometimes leads to a decrease in the degree of myopia. This indicates a positive result of testing the main position of the theory of A.I. Dashevsky about the most important role of accommodation spasm as a trigger in the development of false and axial myopia.
The theory of Otsuca (1967) considers the dependence of the onset and growth of myopia on visual work at close range and the lengthening of the axis of the myopic eyes. The development of myopia is based on the pathological tone of the ciliary muscle, which results in weakness of accommodation, stretching of the choroid, and then the sclera.
This pathological tone of the ciliary muscle is distinguished by the fact that it does not immediately resume after prolonged atropinization. The ciliary muscle (especially the circular fibers of the Müller muscle) gradually atrophies, leading to atrophy of the choroid. At the beginning of the development of myopia, the lens flattens to compensate for the lengthening of the axis, but up to certain limits. Thus, the basis of myopia, according to Otsuka, is the lengthening of the axis of the eye and flattening of the lens.
The only exception is mild myopia, up to 2.0 D, resulting from pathological tone of the ciliary muscle. Tokoro and Suzuki (1968) phacometrically observed the development of myopia in 33 eyes of 18 people suffering from myopia for 7 years. In eyes with lengthening of the axis, a decrease in the refractive power of the lens was observed. These observations confirmed Otsuka's position about the weakening of the lens in myopia.
A. I. Dashevsky (1973), using his objective photo-ophthalmometric research method, comparing the average refractive power of the lens in 163 emmetropic and 400 myopic eyes, confirmed Otsuka’s position on the compensating role of the lens in the early development of myopia. In emmetropic eyes, the refractive power of the lens was 0.61 D (with a significance coefficient t = 2.0) greater than in myopic eyes (22.72 ± 0.03 and 22.11 ± 0.02 D). However, from these data it is clear that the compensatory role of the lens is insignificant.
It should be noted that the mechanism of pathogenesis of elongation of the ocular axis in myopia remains unclear. Accommodation theory of E. S. Avetisov (1965). The author gives accommodation a major role in eye refractogenesis. He believes (1965, 1967) that the state of accommodation regulates the normal formation of the refraction of the eye. If, at the beginning of increased visual load at close range, the ciliary muscle is already formed and can withstand the load, therefore, the refraction is emmetropic or slightly hypermetropic. If by this time the muscle has not yet “matured”, the accommodation is weak, and for visual work at a close distance, a compensatory elongation of the eye develops - myopia (cited by Yu. Z. Rosenblum and N.F. Savitskaya, 1974).
“With a weakened accommodative ability, increased visual work at close range becomes an unbearable burden for the eyes. In these cases, the body is forced to change the optical power of the eyes in such a way as to adapt it to work at close range without straining accommodation. This is achieved mainly by lengthening the anteroposterior axis of the eye during the period of its growth and formation of refraction,” wrote E. S. Avetisov (1975).
In the theory of E. S. Avetisov, three main links can be distinguished:
- 1) visual work at close range - weakened accommodation;
- 2) hereditary conditioning;
- 3) weakened sclera - IOP.
Classification of acquired myopia
. First of all, it is important to fundamentally divide myopia into primary and secondary.
A.I. Dashevsky (1973) described as primary myopia such emmetropia, in which the posterior main plane of the optical system of the eye, shifted slightly anteriorly, caused the eye focus to move slightly anteriorly from the retina of the spherical eye. If there were no such shift in the posterior principal plane and main focus, such an eye would be emmetropic in its anatomical and optical parameters. Developing the ideas of E. J. Tron about the variability of the optical elements of the eyes, the author came to the conclusion that biological variants of emmetropia are possible, caused by different positions of the posterior main plane of the optical system of the eye.
Emmetropia
- the main and most advanced biological version of the norm of clinical refraction. Other variants are caused by displacement of the posterior main plane anteriorly (myopic type of emmetropia) and posteriorly (hypermetropic type of emmetropia). As calculations have shown, many eyes with combinational (according to E. Zh. Tron) ametropia turned out to be such biological variants of emmetropia.
Primary myopia, or the myopic variety of emmetropia, does not exceed 2.0-2.5 D and is stationary. All other types of myopia are:
- 1) hereditary (family);
- 2) congenital;
- 3) symptomatic (transient);
- 4) purchased.
To characterize acquired myopia, it is extremely important to distinguish true (axial) myopia and its secondary strengthening due to the layered spasm of accommodation. We include acquired myopia as early and late pseudo myopia, axial and mixed (axial myopia + accommodation spasm) myopia (Fig. 8).
To create a new classification of myopia, which would reflect the genesis and clinical structure, it was necessary to take into account data from other clinical classifications of progressive myopia.
As can be seen from table. 7, the classification of B. L. Radzikhovsky (1962) is based on three signs: the degree of myopia, the clinical form according to anatomical changes in the fundus and the nature of the development of myopia; E.I. Kuzina (1964), based on the experience of many years of dispensary observation of the condition of myopic eyes, proposed a slightly different clinical classification of secondary (axial) myopia.
This classification is convenient in that it fairly fully presents the clinical characteristics of each case of myopia. Goldschmidt (1968) distinguishes the following types of myopia:
- 1) genetically determined, progressing during growth, rarely exceeding 6.0-9.0 D;
- 2) late, developing for the first time after the cessation of growth, rarely reaching high degrees, depending on the influence of the environment;
- 3) high with long-term degenerative changes in the eyes, in some cases genetically determined, in others genetic factors are of secondary importance, in others - caused solely by environmental influences.
Goldschmidt's recognition of the presence of not only hereditary, but also acquired high myopia coincides with the theory of A.I. Dashevsky.
There are many examples of the development of professional myopia in adults in the literature (P. Ponomarenko, 1956; T. A. Chernitsky, A. G. Sajdakovsky, 1962). The authors believe that myopia in adults is a consequence of the influence of the profession and insufficiently good hygienic conditions. The new clinical classification of acquired myopia that we have developed takes into account the main elements of the classification of refraction by A. I. Dashevsky and the classification of myopia by B. L. Radzikhovsky and E. I. Kuzina. We highlight the type of myopia, genesis, degree of myopia, stage, nature of the anatomical change.
Hereditary, or degenerative, myopia is always familial and is transmitted both by the dominant (Fig. 9) and recessive type (Fig. 10).
Congenital myopia can be a consequence of viral, microbial and other diseases of the mother in the first 3-6 months of pregnancy. Myopia occurs in such cases like other developmental anomalies (Mann, 1947; Badtke, 1952; Frangois, 1973). As is known, congenital myopia does not progress.
Transient myopia
(symptomatic) is not observed so rarely. Transient symptomatic myopia is usually understood as an increase in the refraction of the lens, resulting from the influence of various factors, the main of which are diseases and medications. This type of myopia was described by Horner in the last century in diabetes mellitus.
Transient myopia occurs when taking diuretics, sulfonamides, neuroleptics, ganglion blockers, which can be explained by an allergic reaction (edema) of the ciliary body.
Monkade et al (1967) consider this type of myopia as spastic. They observed her after prescribing supramide and aspirin. Since increased parasympathetic innervation leads to spasm of the accommodative muscle, which is weakened after retrobulbar injection of cocaine, the authors explain this phenomenon by direct irritation of the ciliary muscle. At the same time, they mention as possible reasons a change in the refractive index and a decrease in the production of chamber moisture.
In our classification, the genesis of myopia according to A.I. Dashevsky is completely preserved, changes are made to the distribution of the stage - in the spasmodic stage, early and late pseudomyopia are distinguished, according to clinical experience that showed easy cure for early and difficult cure for late pseudomyonia. In addition, instead of a degenerative stage, an axial complicated one is reflected. In general, the classification covers all types of myopia and reflects in detail the development of acquired myopia (false and axial), taking into account the leading role of accommodation spasm in its genesis.
Our classification of acquired myopia is a stimulus for the doctor to act, since he must determine:
- 1) what kind of myopia occurs - primary or secondary;
- 2) the presence of a spasm of accommodation, transforming emmetropia or hypermetropia into false myopia or, in case of true myopia, increasing its degree (in diopters). The answers to these questions determine the doctor’s treatment tactics.
Prespasms of accommodation.
There are known observations of self-healing accommodation spasms. In this regard, it was suggested that there may be a pre-spasm of accommodation, which mostly disappears on its own, and sometimes turns into an initial spasm. It was already said above that due to the reciprocal relationship between the force of contraction and relaxation of the two antagonistic parts of the ciliary muscle, its absolute rest is impossible. The dynamic balance of a certain tonic contraction of both parts of the muscle is the basis for the contraction of one of them while relaxing the other. When the sympathetic innervation is weakened and parasympathetic innervation prevails, the tone of the Müller muscle is greater than the tone of the Brücke muscle. As the rigidity of the Müller muscle increases, a spasm of accommodation appears.
Our studies have shown that it is not uncommon for visual acuity to be 1.0 at distance, but less than 1.0 at near distance. You can easily find the degree of decrease in visual acuity for close distances using the simple method we have developed. It consists in the following. We place a lens with a power of + 3.0 D in front of the emmetropic eye. This reduces its further point of clear vision with a transition from infinity to a distance of 33.3 cm from the eye. At this distance, with visual acuity equal to 1.0 for distance, you need to read font No. 1 of the Golovin-Sivtsev table for close range or font No. 10 of our table, specially compiled for the described method. If this font is not visible and, therefore, visual acuity for close distance is below 1.0 D, we attach negative lenses, starting from 0.25 and even 0.12 D, to the lens already in front of the eye with a power of +3.0 D. The power of the smallest negative lens that increases visual acuity to 1.0 determines the degree of false myopia for close distance or prespasm of accommodation.
We consider a decrease in distance visual acuity caused by a spasm of accommodation to be a pathology, the beginning of myopia. If there is emmetropia for a distance, and false myopia for a close distance, there is no reason to consider this a pathology. When looking into the distance, such (that is, for a close distance) false myopia disappears, emmetropia for the distance is restored, that is, a normal relationship appears between the antagonists - parts of the ciliary muscle. In healthy eyes in such cases there is a premorbid state.
The above is an explanation of why the true OU of the eye should be considered emmetropic and why in most people it becomes myopic. It substantiates the view of myopic OA in an orientation-free space as a result of adaptation of the accommodative process to environmental conditions.
The occurrence of a spasm of accommodation at close range can be explained as follows. The emmetropic setting is not some kind of optical constant, which is characterized by an exact correspondence between the length of the axis of the eye and the main focal length of its optical system. This setting is the result of a dynamic balance of accommodation for distance and for near distance. When looking into the distance, the lens flattens and the point of clear vision moves further to the distance at which the object in question or a special test object is located. In this case, visual acuity can increase until the maximum resolving power of the eye is reached, the limit of which is limited by the diameters of the cones in the central fovea of the macula.
After applying a lens with a power of +3.0 D in the created myopic system (eye + glass), the stimulus for distance accommodation disappears. As a result, the tone of the two antagonistic parts in the ciliary muscle changes. If, for some reason, the balance of the autonomic innervation of the ciliary muscle is slightly disturbed in the direction of the predominance of parasympathetic activity, then the ratio of the tones of the antagonists of the ciliary muscle for a distance may still be undisturbed (emmetropia), but for a close distance it is already disturbed. Although a lens with a power of +3.0 D provides emmetropic alignment of the eye at a distance, objects visible in peripheral vision create conditions for accommodation at close range.
Thus, in the described spasmodic phenomenon, the beginning of the spasmodic state of the ciliary muscle is manifested for the first time (only for close distance, but not for distance). The occurrence of such incipient rigidity of the ciliary muscle for a close distance is a harbinger of a future spasm when a false myopic refraction appears for a distance. The appearance of a weak, very unstable tension of accommodation for a close distance should be considered a premorbid state in healthy eyes, that is, a pre-spasm of accommodation. We called the detection of pre-spasm and the method for determining this condition a spasmotest.
During a mass examination of schoolchildren, 455 people with emmetropic refraction (910 eyes) were examined for a spasmotest. It turned out that only 34% of people with emmetropia for distance had emmetropia for near distance. In 66% of people with emmetropia, visual acuity for close distance was reduced and with a slight negative correction it increased to 1.0.
During a repeat study six months later, 17 schoolchildren developed a clear spasm of accommodation. In 15 patients, at the first examination, the spasmotest was positive in both eyes, in 2 - in one eye. This fact confirms that the presence of myopia for close distance (with emmetropia for distance) can be considered a condition preceding the occurrence of false myopia for distance. From the experience of our clinic, based on a survey of about 400,000 schoolchildren, it is known that pseudomyopia, unlike true myopia, does not increase with age, but remains at the same level (on average 1-1.5%). The distribution of children with prespasms of accommodation is the same as with pseudomyopia - almost uniform (Table 8).
For comparison, the same study was conducted on soldiers (232 eyes) and 5th year medical students during exams (668 eyes). From the table 9 it follows that the number of children with prespasm of accommodation is less than soldiers and students (Table 10).
The spasmodic phenomenon occurs with various types of refraction. Using a spasmotest, you can identify a spasm of accommodation layered on top of true myopia. With it, the spasmotest may be negative, that is, no increase in refraction is detected. If it is positive, this indicates the initial manifestations of the prevalence of parasympathetic innervation over the sympathetic and the occurrence of prespasm against the background of true myopia, for example, as a harbinger of a relapse of a previously cured spasm of accommodation in this true axial myopia.
As can be seen from the data presented, prespasm of accommodation is a fairly common phenomenon. But if we remember that the spasm of accommodation in some patients disappears without treatment, we can assume that with an improvement in the general condition of the body or a decrease in visual load in the vast majority, the prespasm may disappear temporarily or permanently. This was confirmed by our observations.
A repeated examination of the same schoolchildren revealed the following changes. Of the 442 eyes, 383 were examined after six months. In 96 eyes (25%) there were no changes, in 153 (40%) further myopization was noted for close distance (font No. 1 is visible at a closer distance than before), and in 134 eyes (35%) near myopia decreased, including in 59 eyes it disappeared before near emmetropia was restored (self-healing).
In 29 eyes (9%) in 17 people, as already mentioned, pseudomyopia occurred. These figures give the first idea of the numerical dynamics of prespasm and spasm of accommodation, which, according to mass data from our clinic, are the source of the transition of false myopia to true.
As a result of a simultaneous study of the eye OC and the spasmodic phenomenon (SP) in 400 emmetropic eyes, average values were obtained: OC = 0.73 ± ± 0.29 D and SF = 0.37 ± 0.022 D. In 170 eyes, OC and SF were the same . Out of 230, only in 69 eyes the degree of SF exceeded the degree of OU, in the rest it was less. This can be explained as follows.
The OA itself, if it is not emmetropic, but myopic, represents a change in the initial (natural, that is, emmetropic) state, in which the parasympathetic innervation of accommodation at close range already somewhat predominates.
Myopic OU
- this is already a deviation from the true emmetropic OU and, moreover, a spasmodic deviation. It means that there is something in common between the OA for an orientation-free space (adaptive) and the SF for a close distance, namely, the tendency for accommodation to prevail at a close distance over accommodation at a distance.
If OT and SF are equal to each other, this means that there is no premorbid spasm, there is no pre-spasm of accommodation. If SF is greater than OT, therefore, there is a predominance of parasympathetic innervation for close distance. A stronger SF than OA indicates a true prespasm of accommodation.
Non-drug therapy
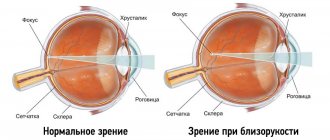
This includes corrective optics - glasses, lenses. Also, to correct vision, simple eye exercises are used, which will be recommended by an ophthalmologist. The fundamental point in myopia is the incorrect focusing of light rays: they do not reach the retina due to changes in the shape of the eyeball and lens
It is important to identify the cause of the enlargement of the lens body, and then fight it
An ophthalmologist may prescribe a course of physiotherapeutic procedures.
With severe swelling of the macula, women may be prescribed medications to remove excess fluid from the body - diuretics. Medicines are selected by a doctor; taking herbs or pills on your own is very dangerous. You should not think that herbal remedies are absolutely safe for the fetus and mother: some herbs cause miscarriages.
Reasons for development
So, let's figure out why such a disease as myopia appears in the first place.
- The occurrence of myopia is determined genetically. Visibility impairment occurs due to an increase in the length of the eyeball, due to which the retina is located outside the focal plane. Each of us has approximately the same length of the eyeball - 24 mm. As the disease develops, the size may increase to 30 mm. Also, the shape of the eye changes to an ellipsoidal one, and both the anterior and posterior axis are lengthened. This phenomenon subsequently provokes stretching of the posterior wall of the eye, as a result of which the fundus of the eye changes.
- A less common phenomenon is the irregular shape of the cornea of the eye, which causes increased focusing of light rays during refraction. The disease most often develops in school-age children and adolescents during the restructuring of the body.
- The disease can also be considered hereditary. Statistics say that half of the parents suffering from myopia also have children with this disease, while among parents without visual impairment, only eight percent of children suffer from myopia.
- In addition, a lack of vitamins and elements in the body such as Zn (zinc), Mn (manganese), Cu (copper) and other minerals can also affect the development of the initial stage of myopia in both eyes.
- Increased strain on vision, poor lighting of the workspace, as well as incorrect posture when working with objects at close range are the main causes of myopia in schoolchildren and students.
- Myopia can also develop as a result of a hormonal imbalance that occurs in the body.
- Past infections can also trigger the disease.
- Myopia can be a consequence of birth trauma.
- Another reason: cerebrovascular dysfunction and intracranial hypertension.
- The weakened accommodative function leads to the fact that the eyeball increases in length.
- The cause of myopia is also incorrect vision correction - deterioration can be caused by incorrectly selected glasses or contact lenses.
Diagnostics
To identify myopia, contact an ophthalmologist who conducts a visual examination and other diagnostic measures.
Before treating mild myopia, a number of diagnostic techniques are performed. They are reflected in the table.
| Method of diagnosis. | Description. |
| Visometry. | Vision test according to the table. |
| Ophthalmoscopy. | Fundus examination. |
| Tonography. | Checking the outflow of intraocular fluid. |
| Perimetry. | Determination of visual fields. |
| Ophthalmometry. | Determination of the optical power of the corneal layer of the eye. |
| Skiascopy. | Study of shadow movement in the pupil area. |
| Refractometry. | Testing the eye's ability to reflect light rays. |
| Tonometry. | Determination of intraocular pressure. |
| Ultrasonography. | Determining the length of the eyeball to determine possible pathology. |
Read in a separate article: How to get rid of myopia at home
If after research it turns out that a person actually has a diagnosis of “low myopia,” then appropriate treatment is prescribed.
Treatment of mild myopia
Treatment includes the use of several therapies, depending on the degree of disease progression. If mild myopia is diagnosed, treatment is carried out using conservative methods. Vitamins are prescribed as healing drugs:
- A - promotes normal functioning of the retina;
- B1 - regulates metabolism in the body;
- B2 - relieves eye tension;
- ascorbic acid - helps strengthen the sclera of the eyes;
- nicotinic acid - improves blood circulation, dilating blood vessels.
These drugs are available for oral administration and as eye drops. To strengthen the blood vessels and walls of the structure of the organs of vision, medications containing calcium are prescribed:
This visual problem causes nearby objects to be clearly visible, but distant objects to be blurred. This is due to an increase in the anteroposterior diameter of the eye. Accustomed to innate ones. This may be accompanied by an increase in the curvature of the cornea or one or both sides of the lens. This is due to late acquired myopia.
It is provoked by a change in the refractive index of the aqueous or vitreous body. Usually this is acquired senile myopia. In the vast majority of cases and generally in the most intense forms, myopia is of the axial type. Myopia is clinically classified as benign or simple myopia and pathological or degenerative myopia.
- Trental;
- Rutin;
- Calcium gluconate.
To prevent eye spasm, use drops: Mezaton, Irifin. Physiotherapeutic procedures help stop the development of pathology.
First degree myopia can be treated with laser eye correction. This modern operation reduces the curvature of the cornea using strong radiation. Pathology of mild and moderate severity can be corrected. In preparation for surgery, a thorough examination of the condition of the cornea of the eye is carried out.
Simple myopia is a condition of limited progression in which the refractive error does not exceed 6 diopters and does not cause problems in the day. On the contrary, with pathological myopia the process is obviously more serious, since the fundus changes. In this case, the refractive index exceeds 6 diopters, and the pathology can rapidly increase to such an extent that it deserves attention as a separate clinical entity. The etiology of pathological myopia is not entirely clear. In general, scleral weakness and its subsequent inability to withstand intraocular pressure without recoil and expansion were addressed.
All data is entered into a computer, which makes calculations for the operation. The procedure is carried out on the basis of a developed program, so the risk of error is minimized. The patient is instilled with drugs to relieve sensitivity and dilate the pupil, the head and eyelids are fixed, and the necessary incisions are made to the cornea.
Fund changes have been recognized as being caused by this stretching, but most likely they are usually associated with a genetic developmental defect that affects the entire posterior segment of the eye. Whatever the cause, it is likely that the main disadvantage of myopia is developmental change. Thus, this seems to point to the fact that this process, although rarely congenital, can occur early and is usually hereditary.
We can say that myopia develops only during the period of active growth of a person, since elongation of the eye, which remains at normal size until the age of 25, is very rare. The eye shares with the brain the characteristic of growing earlier than the rest of the body, and by age 20 the eye and brain have already reached their adult size. It has been suggested that myopia is a consequence of the continuity of this prematurity due to the lack of a moderating influence.
The operation lasts a few minutes, then the patient returns home. After the procedure, you must follow all the doctor’s instructions: drop antibiotics into your eyes, sleep only on your back in the first days, and maintain eye hygiene. This manipulation allows you to cure myopia and restore eye vigilance.
Symptoms
At first, mild myopia does not manifest itself much. But as vision deteriorates below one and a half diopters, discomfort begins to appear when viewing distant objects.
Symptoms indicating low myopia are as follows:
- constant eye fatigue;
- you have to squint to look at distant objects;
- when reading or writing, there is a desire to bend over or get closer to the object in question;
- feeling of sand in the eyes after prolonged strain;
- dryness and redness of the organs of vision.
The presence of one or more signs for a long time is a reason to visit an ophthalmologist.
Classification of myopia
The disease is divided into several types and stages, depending on the degree of refractive error:
- Progressive. Visual acuity is constantly falling, every year the indicator worsens by at least one diopter. Such rates of progression of the disease can lead to serious problems;
- Transitional. There is a temporary impairment of visual acuity due to external or internal negative factors. Such myopia is often diagnosed in pregnant women in the first trimester. For this reason, a re-examination by an ophthalmologist is required after some time;
- Stationary. Myopia does not progress and is usually characterized by minor deviations in refraction. The pathology can be eliminated using corrective optics.
Myopia does not have a negative impact on pregnancy, but may worsen during childbirth.
Based on the degree of refractive error, the disease is divided into the following categories:
- Easy. Negative symptoms are practically not felt. Objects located at a distance acquire a blurred outline. In some cases, migraines appear. The first sign of a decrease in visual acuity is that a person constantly squints to look at distant objects. Deviations in refraction are no more than three diopters. With weak myopia, a pregnant girl is prescribed special gymnastics, and natural childbirth is allowed;
- Average. A serious deviation from the norm that negatively affects the quality of daily life and professional activity. However, a timely visit to the doctor will help correct the pathology with the help of properly selected lenses or glasses. Moderate myopia is detected between the ages of twenty-five and thirty years. Deviations in refraction range from three to six diopters; without corrective optics, objects at a distance are practically invisible;
- Heavy. Visual acuity drops from six to thirty diopters. The patient is not able to see even those objects that are located in close proximity to him. The pathology can occur without serious deviations, but is sometimes accompanied by detachment of the retina. In severe myopia, a cesarean section is recommended to eliminate the risk of hemorrhage during natural childbirth. A pregnant woman should be seen regularly by an ophthalmologist.
Symptoms of myopia
The main symptom of a pathology such as myopia is a decrease in distance visual acuity
, distant objects appear blurry. To look at objects located at a certain distance, a person begins to squint, trying to focus.
How does a person with myopia see?
Myopia may be accompanied by the following symptoms and diseases:
- Often, due to the habit of squinting, overstrain of the eye muscles
, which is the cause of the development of asthenopia. - Astigmatism
. In this case they talk about myopic astigmatism. - Tired eyes
, feeling of tension. - Headache.
Causes of 1st degree myopia
Myopia can develop under the influence of many external and internal factors. The disease is often diagnosed in adolescents, since they receive a heavy load on the organ of vision not only in school, but also at home. From eighteen to forty-five years, the disease remains stationary, i.e. not progressing.
Heredity
It has been scientifically proven that myopia develops more often in children whose parents suffered from a similar anomaly. If the father or mother is nearsighted, then in 50% of cases the child will also have vision problems. At the same time, in babies born from healthy parents, the risk of encountering myopia is extremely low (only 10%).
Remember that children do not “inherit” the pathology itself, but only a physiological predisposition.
Lack of microelements
A deficiency of important minerals such as zinc, copper or manganese can cause myopia. These substances play a huge role in the photochemical processes occurring in the visual apparatus, more precisely, in the retina of the eye.
Violation of hygiene requirements
Myopia of the first degree can be caused by prolonged eye strain, long-term work at a short distance, reading in low light, excessive involvement with computers and watching TV programs.
Often a harbinger of pathology is a spasm of accommodation, which causes a strong and prolonged load on the visual apparatus
At the first stage, it is important to adjust your lifestyle and provide more rest to your eyes
Past infections
The risk group includes people who have had measles, diphtheria, viral hepatitis, and tuberculosis. Diseases of the nasopharynx (sinusitis) and oropharynx (tonsillitis) play a significant role in the progression of myopia.
Hormonal imbalances
Pathology can develop rapidly in patients with reduced immunity and disorders of the endocrine system. Myopia of the first degree can develop against the background of hormonal changes in the body. For this reason, the disease is often diagnosed in adolescents and pregnant women.
Birth injuries
In newborn babies, pathology manifests itself as a result of damage to the spine during childbirth. Also, the cause of myopia in children is excessive extensibility of the sclera or its weakness, the intensive growth rate of the child.
Anatomical certificate
The cornea and lens are the main structures that are involved in the refraction of light and transmission of images to the retina. The lens is suspended on thin ligaments, which are fixed to the ciliary (ciliary) muscle.
When this muscle relaxes, the ligaments tighten, the lens flattens in response and its refractive power decreases. And vice versa: contraction of the ciliary muscle relaxes the ligaments and makes the lens more convex, resulting in an increase in its refractive power. This mechanism is called accommodation. Thanks to it, a healthy person perceives objects equally well both at close and far distances.
Thanks to the lens and accommodation, the image falls on the retina. Light impulses react with light-sensitive cells in the retina and enter the brain, where visual images are formed. For the image to be clear, the image must be projected strictly onto the retina.
The higher the degree of myopia, the shorter the distance from which a person can see well
With myopia (myopia), certain disturbances occur in the accommodation system, as a result of which the image is projected not on the retina, but in front of it. It is for this reason that a person sees objects located at a distance blurry. The higher the degree of myopia, the shorter the distance from which a person can see clearly. Readers often wonder: “Is myopia a plus or a minus?” The answer is simple: Myopia is a minus. And it is indicated in the doctor’s prescription as: Sph - 1.5D (The value -1.5; -2 or another indicates the optical power of the lens)
Varieties
It is important not only the degree of the disease, but also the determination of its type. Based on the nature of its occurrence, myopia is divided into:
- to a landline. The identified pathology does not worsen over time;
- progressive. Vision is steadily declining. Every year it decreases by about one diopter;
- malignant. It is not so much a refractive error as a severe type of disease that quickly leads to disability. A person loses the ability to perform usual professional and everyday activities.
Diagnostics
Mild myopia may initially not manifest itself in any way and may not affect the quality of life. To determine the pathology and take timely corrective measures, you need to visit an ophthalmologist annually. The level of acute vision is checked using Sivtsev or Golovin tables. For young children, a specially designed Orlova table is sometimes used. Surveys are carried out using:
ophthalmoscopy. Allows you to evaluate the retina, optic nerve head, and fundus vessels. With the advent of retinophot, you can not only examine, but also get a high-quality image;- skiascopy. “Shadow test” occurs by illuminating the pupil with a beam of light reflected from the mirror. The position of the spatial optical phenomenon depends on the refraction of the eye being examined;
- refractometry. A non-invasive objective diagnostic method that allows you to determine abnormal changes in the refractive power of the eye, leading to various diseases;
- ophthalmometry. Determines the radius of curvature of the cornea, which is involved in ensuring visual acuity along with other elements of the optical system of the eye. It is carried out by three methods: manual, mechanical and using a computer;
- keratotopography. Allows you to study in detail the condition of the cornea of the eye. The result of the scan is a color map of its surface;
- Ultrasound of the eye, or ophthalmoechography. Allows a detailed study of the structures of the ocular apparatus. The technique is considered highly informative because it provides a detailed image of the orbit on a computer monitor.
How to restore and improve vision with myopia?
Is it possible to restore sharpness and clarity of vision using some conservative means? How to improve vision for myopia in teenagers? You can restore your vision without surgery and without taking medications using our instructions. Vision, the structure of the eye, is such a complex system that it will not be possible to completely restore anything there. It can be supported, it can be improved, but even laser correction does not provide a complete guarantee of irrevocable recovery.
Get laser correction
Unfortunately, this type of surgery does not cure vision. It corrects focus, but it will not help stop progressive myopia in teenagers. Over time, vision may begin to decline again. If vision rapidly decreases, it means that there is some kind of disturbance in the structure of the eye, or the reason may be even deeper. How many cases have there been of loss of vision from diabetes, from a tumor in the brain?
The most important thing in treating any disease is to find the correct cause of the disease. Only then will all attempts to restore good vision to a teenager be effective
Start eating right
For some reason everyone neglects this point. Can myopia in teenagers be treated by changing their diet? No, but without adjusting it and taking certain vitamins and medications, treatment will be more difficult. The eyes love carrots, and blueberries are very useful for them. So why not give this simple method of maintaining good vision a chance?
Correction of moderate myopia: how to treat?
There are various correction methods, including without surgical intervention. Each has its own pros and cons, as well as contraindications. Treatment for myopia is selected individually by the doctor only after a complete examination.
Correction with lenses
Doctors use three types of lenses for optical correction:
- Contact lenses. They can be soft or hard. You cannot select contact lenses yourself, since it is not enough to know their optical power and radius. Depending on the type, one pair of lenses can be worn from 1 to 30 days.
- Night o-lenses. These optical products appeared in Russia relatively recently, so few people know about their existence. The principle of the effect of ortholenses is based on the gradual shifting of the corneal epithelium, as a result of which, after removing the lenses, a person sees well for 12-48 hours. They should only be worn at night. One pair can be used for 12 months.
- Phakic lenses. They are implanted directly into the eye through a minor surgical operation.
Night ortholenses are considered the most effective because they cause minimal discomfort when worn and stop the progression of myopia.
Hardware correction
Hardware correction gives good results with regular use. It is most often prescribed to children, but this technique is also used for adults. This is one of the most effective non-invasive techniques.
“Visotronic”
This is a special simulator with an electronic control module; it includes three main programs and the same number of additional ones. The therapeutic effect is based on training the oculomotor and ciliary muscles.
During treatment, the patient looks at tables and moving images.
The course of therapy is from 10 to 20 sessions.
“Stream”
The device is designed to relieve spasm of accommodation. The control is an electronic unit, which contains 6 programs + 2 auxiliary ones.
During therapy, the patient observes symbols approaching and receding. The backlighting of numbers and figures can change from red to green and back.
The course includes 10 sessions.
Diagnostic features
To prescribe the optimal therapeutic course, the doctor must conduct a diagnostic examination. Moreover, the sooner it is carried out, the greater the chances of timely identification of the cause of the pathological condition and successful treatment. Therefore, you should consult a doctor immediately after the first suspicious symptoms appear, for example, decreased visual acuity or redness of the eyes. First of all, the ophthalmologist will study the patient’s complaints and check his vision using a special table with letters.
At an appointment with an ophthalmologist
In addition, the doctor may prescribe additional diagnostic procedures:
- visual field test;
- ultrasound examination (ultrasound);
- skiascopy (determining the refraction of the patient’s eye);
- biomicroscopy of the eye;
- examination of the fundus using a slit lamp.
Diagnostic methods
Based on the test results, the doctor will be able to make an accurate diagnosis and prescribe appropriate treatment. The course of therapy is prescribed taking into account many factors, including the individual characteristics of the patient, his age, the severity of the disease and the presence of allergies to medications.